






















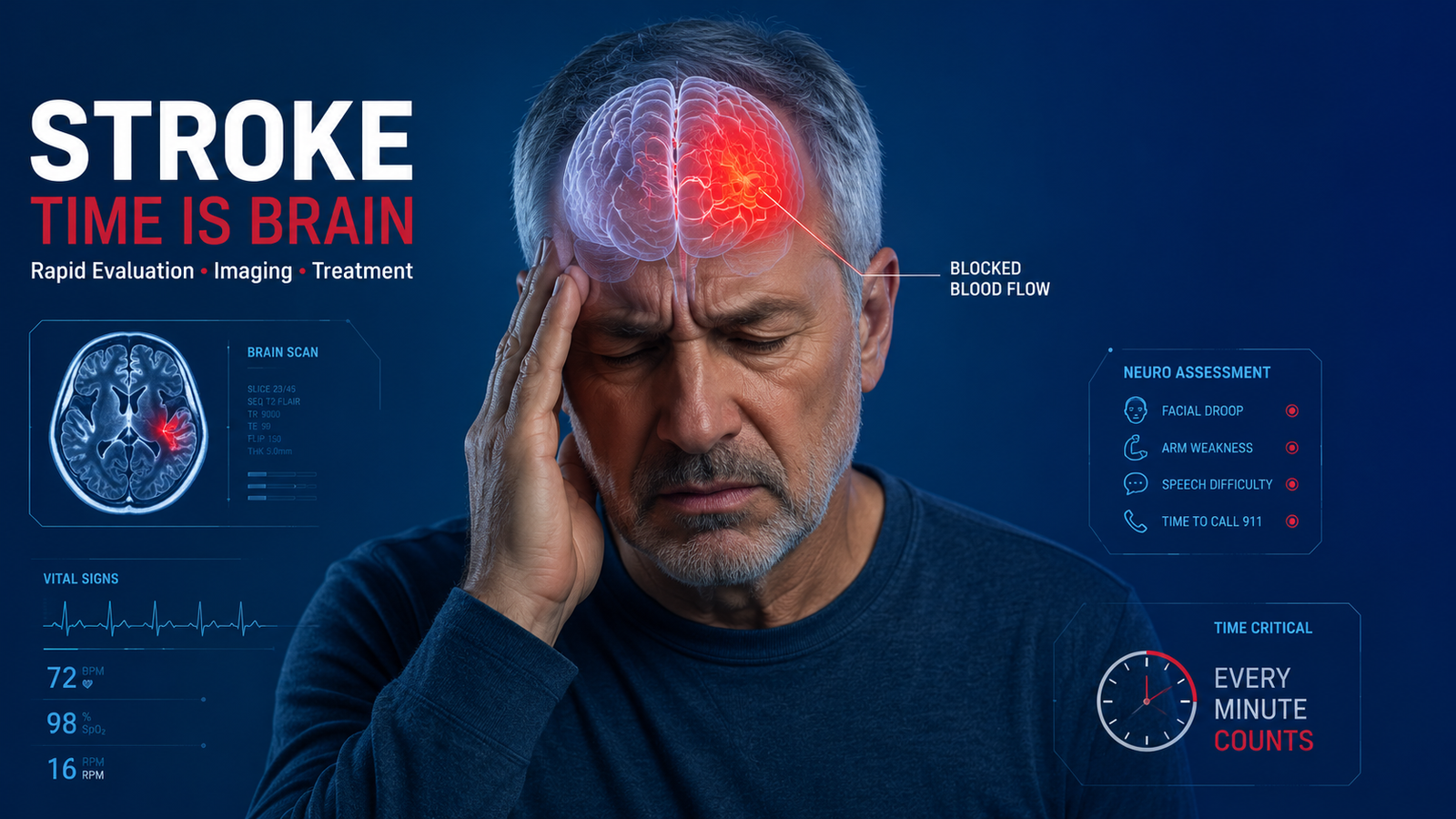
Stroke: Evaluation and Treatment — 9 Critical Steps That Save Lives
Stroke: Evaluation and Treatment — 9 Critical Steps That Save Lives Stroke evaluation and treatment is a race against the clock. When brain ischemia strikes,

Neurology Consultation: 15 Signs to Make an Appointment at Consultant Corner in Bloomington, IL and El Paso, TX
Neurology Consultation: 15 Signs to Make an Appointment at Consultant Corner in Bloomington, IL and El Paso, TX A neurology consultation is one of those
Neurological Care: 10 Reasons Patients Choose Consultant Corner in Bloomington, IL & El Paso, TX
Neurological Care: 10 Reasons Patients Choose Consultant Corner in Bloomington, IL & El Paso, TX Most people don’t think about neurology until they have a