
Epilepsy and Seizures: 10 Important Facts
Epilepsy and Seizures: 10 Important Facts Epilepsy and seizures are among the most misunderstood neurological conditions in the United States, yet they affect millions of people across every age group. Epilepsy and seizures don’t discriminate by background, but research shows the disease is more common in certain age groups, and its severity often depends on a person’s overall health, access to care, and how quickly the condition is diagnosed. Whether you or a loved one has just experienced a first seizure, or you’ve been living with an epilepsy diagnosis for years, understanding the facts can help you make smarter, calmer decisions about treatment and long-term brain health. At Consultant Corner, we work with patients across the country who are navigating a new epilepsy diagnosis or trying to get long-standing seizures under better control. Below are 10 important facts everyone should know about epilepsy and seizures — backed by current medical understanding and practical guidance from our neurology team. 1. Epilepsy Is More Common Than Most People Realize According to the Centers for Disease Control and Prevention, about 1.2% of the U.S. population — roughly 3.4 million people — currently has active epilepsy. That makes it one of the most common neurological disorders in the country, alongside conditions like migraine and stroke. Despite how common epilepsy and seizures actually are, public understanding lags far behind the statistics. Many people picture only the most dramatic convulsive seizures when they think of epilepsy, when in reality the condition shows up in dozens of subtler forms — brief staring spells, sudden confusion, repetitive movements, or even unusual emotional surges that last only seconds. Because these milder presentations don’t match the popular image of epilepsy, they’re frequently missed, dismissed, or misattributed to anxiety, fatigue, or simple distraction. This gap between perception and reality is part of why early diagnosis is so often delayed — sometimes for years. Why this matters: Epilepsy and seizures are far more prevalent than the public conversation around them suggests, which means stigma and misinformation often outweigh actual medical understanding. The more people understand how common — and how varied — seizures can look, the faster real cases get identified and treated. 2. Epilepsy and Seizures Affect Certain Age Groups More Than Others Epilepsy and seizures tend to cluster at two points in life: early childhood and older adulthood. Children under 2 and adults over 65 have the highest rates of new epilepsy diagnoses, while the years in between generally carry a lower — though not zero — risk. In children, many epilepsy cases are linked to genetic factors, developmental conditions, or fevers during early brain development. Pediatric epilepsy often responds very well to treatment, and a significant number of children eventually outgrow certain seizure syndromes entirely as their brains mature. In older adults, the picture looks different. New-onset seizures after age 65 are frequently linked to prior strokes, head injuries, or brain changes associated with aging — which is why patients recovering from an ischemic stroke or an intracerebral hemorrhage are routinely monitored for seizure activity during follow-up care. Unlike in children, epilepsy that develops later in life is less likely to resolve on its own and more often requires long-term medication management. This age-based pattern is one of the clearest illustrations of how epilepsy and seizures are shaped by what’s happening elsewhere in a person’s health — whether that’s a developing brain or one recovering from injury. 3. A Seizure Is Not Always Epilepsy One of the most important distinctions in neurology: a single seizure does not automatically mean someone has epilepsy. Epilepsy is generally diagnosed only after a person has had two or more unprovoked seizures, or one seizure combined with a high risk of recurrence based on EEG or imaging findings. Provoked seizures — caused by fever, low blood sugar, alcohol withdrawal, severe dehydration, or a head injury — are treated very differently than epilepsy itself. A provoked seizure is treated by addressing the underlying trigger (correcting blood sugar, managing withdrawal, treating the fever), and once that trigger is resolved, the person may never need long-term anti-seizure medication at all. This distinction matters enormously for patients, because a single seizure understandably feels frightening and can lead people to assume the worst. A thorough neurological workup — including bloodwork, brain imaging, and often an EEG — helps determine whether what happened was an isolated, provoked event or the first sign of a chronic seizure disorder. Jumping to conclusions in either direction, either dismissing a first seizure as “nothing” or assuming permanent epilepsy after one event, can lead to the wrong care path. 4. There Are Many Different Types of Seizures Seizures are broadly divided into two categories — focal and generalized — but within those categories, presentations vary widely from patient to patient. Seizure Type Description Common Signs Focal (Partial) Seizures Start in one area of the brain Twitching, unusual sensations, brief confusion, staring spells Generalized Seizures Involve both sides of the brain Convulsions, loss of consciousness, muscle stiffening, falling Absence Seizures Brief lapses in awareness Blank staring, subtle eye fluttering, usually in children Tonic-Clonic Seizures Most recognized “grand mal” type Body stiffening followed by jerking movements Myoclonic Seizures Sudden brief muscle jerks Quick jerks of arms or legs, often clustered Atonic Seizures Sudden loss of muscle tone Limp collapse or head drop, brief loss of posture Recognizing the type of seizure a person experiences is critical, because treatment plans and medications differ significantly between seizure types. A medication that works well for tonic-clonic seizures may do little for absence seizures, and vice versa. This is one of the main reasons self-diagnosis or guessing at treatment based on general epilepsy information online can backfire — accurate classification usually requires a detailed history and, ideally, EEG monitoring that captures the brain’s electrical activity during an actual event. 5. Severity Often Depends on Overall Health Epilepsy and seizures don’t impact every patient equally. Severity, frequency, and recovery time are strongly influenced by a person’s underlying health — including cardiovascular
Multiple Sclerosis Symptoms and Treatment: 11 Essential Facts

Multiple Sclerosis Symptoms and Treatment: 11 Essential Facts Multiple Sclerosis symptoms and treatment are two of the most searched topics among Americans who notice unexplained numbness, vision changes, or fatigue that simply won’t go away. Multiple Sclerosis (MS) can look different in nearly every patient, which makes it one of the more confusing neurological conditions to recognize early. Whether you’re trying to make sense of a new symptom, supporting a loved one through diagnosis, or seeking a second opinion on an existing treatment plan, understanding the facts about MS symptoms and treatment can help you make confident, informed decisions about your health. At Consultant Corner, our neurology team works with patients at every stage of this disease — from the very first unexplained symptom through decades of long-term management. Below are 11 essential facts everyone should know about Multiple Sclerosis symptoms and treatment, explained in plain language so you understand exactly what’s happening in your body and what choices are available to you. Fact 1: MS Is an Autoimmune Disease, Not an Infection Multiple Sclerosis develops when the immune system mistakenly attacks myelin, the protective coating that wraps around nerve fibers in the brain, spinal cord, and optic nerves. When myelin is damaged, nerve signals slow down or stop entirely, which produces the wide variety of symptoms associated with MS. This is fundamentally different from an infection or contagious illness — MS cannot be “caught” from another person, and it is not caused by a virus or bacteria in the way a cold or flu would be. Researchers believe a combination of genetic predisposition and environmental triggers, such as prior viral infections or low vitamin D exposure, plays a role in who eventually develops the disease. Fact 2: Multiple Sclerosis Symptoms Vary Dramatically From Person to Person One of the reasons MS is so difficult to self-diagnose is that Multiple Sclerosis symptoms rarely look the same in two people, even within the same family. Common early signs include: Numbness or tingling, often in the face, arms, legs, or torso Electric-shock sensations that run down the spine when bending the neck Blurry, double, or partially lost vision, sometimes with eye pain Balance problems or a feeling of unsteadiness when walking Muscle weakness or stiffness, particularly in the legs Fatigue that does not improve with rest or sleep Brain fog, slowed thinking, or short-term memory trouble Bladder urgency, frequency, or occasional incontinence Muscle spasms or involuntary twitching Sensitivity to heat, which can temporarily worsen existing symptoms These symptoms can appear suddenly in episodes called relapses, or they can build gradually over months or years. Because many of these symptoms overlap with other common conditions like vitamin deficiencies, anxiety, or chronic fatigue syndrome, patients often go through a lengthy diagnostic process before MS is confirmed. Fact 3: There Are Four Recognized Types of MS Neurologists classify Multiple Sclerosis into four main categories, each with a different pattern of progression. Understanding which type you may have helps your care team choose the most effective treatment strategy. MS Type Pattern of Disease Typical Course Relapsing-Remitting MS (RRMS) Flare-ups followed by partial or full recovery Most common type, especially at diagnosis Secondary Progressive MS (SPMS) Begins as RRMS, then steadily worsens Usually develops years after initial RRMS diagnosis Primary Progressive MS (PPMS) Gradual, continuous worsening from the start No distinct relapses or remissions Clinically Isolated Syndrome (CIS) A single episode suggestive of MS May or may not develop into full MS You don’t need to know which type you have before seeking help — a neurologist will determine this through clinical evaluation, imaging, and ongoing monitoring over time. In many cases, the classification can shift as the disease evolves, which is another reason consistent specialist follow-up matters so much. Fact 4: Age and Demographics Influence MS Risk Multiple Sclerosis most commonly appears in adults between 20 and 40 years old, although it can be diagnosed in children, teenagers, or older adults as well. In the United States, MS is roughly two to three times more common in women than men, a disparity researchers continue to study in relation to hormonal and immune system differences. MS also tends to be diagnosed more frequently in people of Northern European descent, though it affects people of every racial and ethnic background, and recent research suggests Black Americans may experience more aggressive disease courses on average. Geography plays a role too. Areas farther from the equator, including much of the northern United States, tend to report higher MS rates — a pattern researchers associate with lower vitamin D levels from reduced sunlight exposure during childhood and adolescence. This is sometimes referred to as the “latitude gradient” in MS epidemiology. Fact 5: Severity Often Reflects Overall Health and Lifestyle The severity and progression of Multiple Sclerosis symptoms and treatment outcomes are closely tied to a patient’s general health. Smoking, obesity, poorly managed cardiovascular conditions, and chronic, unmanaged stress have all been associated with faster disease progression and more frequent relapses. Comorbid conditions such as diabetes or high blood pressure can also complicate MS management and accelerate disability if left unaddressed. On the other hand, patients who maintain regular physical activity, balanced nutrition, adequate sleep, and consistent medical follow-up often experience more stable, manageable disease courses. This is one of the most important — and often overlooked — facts about living with MS in America today: your daily habits genuinely influence how the disease behaves over time, alongside whatever medication plan your neurologist recommends. Fact 6: MRI Imaging Is the Cornerstone of Diagnosis Because MS symptoms overlap with many other neurological conditions, diagnosis isn’t based on symptoms alone. Magnetic Resonance Imaging (MRI) allows neurologists to see lesions, or areas of damaged myelin, in the brain and spinal cord. A spinal tap (lumbar puncture) and blood tests are sometimes used to rule out conditions with similar presentations, such as vitamin B12 deficiency, lupus, neuromyelitis optica, or other autoimmune disorders. According to the National Institute of Neurological Disorders and Stroke, accurate diagnosis typically
Parkinson’s Disease Explained: 8 Early Symptoms to Watch For

Parkinson’s Disease Explained: 8 Early Symptoms to Watch For Parkinson’s disease symptoms rarely show up all at once. Most people notice one small change first — a slight tremor in a finger, a button that’s harder to fasten, handwriting that’s gotten smaller, or a walk that feels a little slower than it used to. Because these changes are gradual, it’s easy to brush them off as “just getting older.” But recognizing Parkinson’s disease symptoms early can make a real difference in how the condition is managed and how long someone stays independent and active. At Consultant Corner, we evaluate patients across the country who are noticing these subtle shifts, and one thing we hear again and again is, “I wish I had come in sooner.” This guide walks through the eight early warning signs of Parkinson’s disease, who is most at risk, what causes the condition, and how a movement-disorder specialist approaches diagnosis and treatment. If you’re also exploring related topics, you may want to read our companion piece, Understanding Essential Tremor vs. Parkinson’s Disease, which explains how to tell these two conditions apart. What Is Parkinson’s Disease? Parkinson’s disease is a progressive neurological condition that develops when dopamine-producing brain cells gradually decline. Dopamine is a chemical messenger that helps coordinate smooth, controlled movement. As dopamine levels drop, the brain has a harder time sending the right signals to the muscles, which is why Parkinson’s disease symptoms so often show up as tremor, stiffness, and slowed movement. It’s worth noting that not every tremor or every slow movement points to Parkinson’s. Several other conditions can look similar, including essential tremor, drug-induced movement disorders, atypical Parkinsonism (such as PSP, MSA, or CBD), gait disorders, restless leg syndrome, and post-stroke movement disorders. This is exactly why a proper neurological evaluation matters — self-diagnosing from a list of symptoms online can lead to unnecessary worry or, just as often, false reassurance. According to the National Institute on Aging, Parkinson’s disease most commonly develops after age 60, though younger-onset cases do occur. Risk and severity in the United States can vary based on age, genetics, environmental exposures, and overall health, which is part of why personalized evaluation is so important rather than relying on a generic checklist. Who Is Most at Risk? Age is the single biggest risk factor for Parkinson’s disease. Most people are diagnosed after age 60, and risk continues to climb with each decade after that. Men are diagnosed somewhat more often than women. A family history of Parkinson’s, certain genetic mutations, and long-term exposure to specific pesticides or industrial chemicals have also been linked to higher risk. Severity and progression vary widely from person to person. Two people diagnosed at the same age can have very different experiences — one may have mostly mild tremor for years, while another may notice faster changes in balance and mobility. Overall health, including cardiovascular health, activity level, and how quickly symptoms are identified and treated, plays a meaningful role in how the disease progresses. 8 Early Symptoms of Parkinson’s Disease Below are the eight early signs that most often prompt people to schedule an evaluation. 1. Tremor at Rest A tremor that appears when the hand is relaxed — not when it’s being used — is one of the most recognizable Parkinson’s disease symptoms. It often starts in just one hand or even a single finger and may look like a slight rhythmic shaking, sometimes described as a “pill-rolling” motion. 2. Slowed Movement (Bradykinesia) Bradykinesia means movements take noticeably longer to start and complete. Simple tasks like buttoning a shirt, tying shoes, or getting up from a chair may begin to feel unusually slow or effortful. 3. Stiffness in Arms, Legs, or Neck Muscle stiffness, sometimes called rigidity, can limit range of motion and make the body feel tight or resistant to movement. It’s frequently mistaken for arthritis or a pulled muscle before a neurological cause is considered. 4. Balance Problems or Frequent Falls As Parkinson’s affects the brain’s coordination signals, balance can become unsteady. Frequent stumbling, near-falls, or actual falls — especially without an obvious trip hazard — deserve attention. 5. Shuffling Gait or Reduced Arm Swing A walking pattern that shifts to smaller, shuffling steps, a stooped posture, or one arm that swings less than the other while walking are classic early motor signs. Some people also describe sudden “freezing” episodes where their feet feel stuck to the floor mid-step. 6. Sleep Disturbances Acting out vivid dreams, thrashing, or talking during sleep — a condition called REM sleep behavior disorder — can actually appear years before motor symptoms develop. It’s one of the more overlooked early indicators. 7. Loss of Smell A reduced or lost sense of smell (anosmia) that isn’t explained by a cold or sinus issue is a surprisingly common early non-motor symptom of Parkinson’s disease. 8. Mood and Cognitive Changes Anxiety, depression, loss of motivation, or new difficulty concentrating can all show up before noticeable movement changes. Constipation, bladder issues, and lightheadedness when standing are also part of this non-motor symptom cluster. A Quick Note on Timing These non-motor symptoms often appear well before a formal diagnosis is made. Recognizing the pattern — rather than waiting for a single dramatic symptom — is often what leads to earlier, more effective treatment. Motor vs. Non-Motor Symptoms at a Glance The table below summarizes the difference between the two main symptom categories. Symptom Category Examples Why It’s Often Missed Motor Symptoms Tremor at rest, bradykinesia, stiffness, shuffling gait, balance issues Mistaken for normal aging or arthritis Non-Motor Symptoms Sleep disturbances, loss of smell, anxiety/depression, constipation, lightheadedness Not commonly associated with a movement disorder Cognitive Symptoms Memory or concentration problems Attributed to stress or aging Autonomic Symptoms Bladder issues, blood pressure drops on standing Often treated separately by other specialists Why Early Diagnosis of Parkinson’s Disease Matters Identifying Parkinson’s disease symptoms early gives both the patient and the care team more options. Early evaluation allows a movement-disorder specialist to: Start
Alzheimer’s Disease: Early Symptoms Every Family Should Know

Alzheimer’s Disease: Early Symptoms Every Family Should Know Recognizing Alzheimer’s disease early symptoms can make the difference between a family caught off guard and a family prepared with a plan. Memory loss is often dismissed as “just getting older,” but when forgetfulness starts interfering with conversations, appointments, familiar routines, or personal safety, it may be one of the earliest warning signs of Alzheimer’s disease or a related condition. This disease is more common in certain age groups, and its severity often depends on the overall health of the individual — a pattern seen consistently across the United States, where Alzheimer’s remains one of the leading causes of cognitive decline in older adults. This guide walks through the Alzheimer’s disease early symptoms every family should watch for, the conditions that can mimic memory loss, why early diagnosis matters so much, and how a neurology team like Consultant Corner can help you find clarity instead of guesswork. Is Forgetfulness Starting to Impact Daily Life? Occasional forgetfulness — misplacing your keys or forgetting a name for a moment — is normal. But when memory lapses begin to disrupt daily routines, relationships, or independence, it’s worth paying closer attention. What feels like “normal aging” may actually be an early sign of Alzheimer’s disease, Mild Cognitive Impairment (MCI), or another neurological condition entirely. The earlier these changes are evaluated, the more options families have. Early evaluation can slow decline, protect independence, and give families the clarity they need to plan ahead with confidence. If you’re also noticing changes in mood or sleep alongside memory issues, our article on Sleep and Brain Health: What’s the Connection? explains how poor sleep can accelerate cognitive symptoms. Red Flags You Should Never Ignore Understanding the Alzheimer’s disease early symptoms means knowing what falls outside the range of typical aging. If you notice any of the following patterns, a neurological evaluation is recommended. Memory Changes Forgetting recent events or conversations shortly after they happen Misplacing items in unusual places and being unable to retrace steps to find them Relying heavily on notes, reminders, or family members to recall information they used to know easily Thinking & Communication Problems Trouble finding the right words during conversation Repeating the same questions within a short period of time Difficulty following conversations, especially in groups or noisy settings Daily Function Decline Problems managing bills, medications, or appointments that were once handled with ease Getting lost in familiar places, including neighborhoods lived in for years Behavioral or Mood Changes Irritability, anxiety, depression, or social withdrawal Suspicion, paranoia, or uncharacteristic decision-making These early warning signs often appear months or even years before a clear diagnosis is made. That’s part of what makes Alzheimer’s disease early symptoms so easy to overlook — they build gradually rather than appearing all at once. Why subtle signs matter A single forgotten appointment isn’t a red flag. A pattern of forgotten appointments, repeated questions, and difficulty managing routine tasks over several months is. Tracking patterns, rather than isolated incidents, is one of the most useful things a family can do before a medical visit. Memory Loss Isn’t Always Alzheimer’s One of the most important things to understand is that Alzheimer’s disease early symptoms can overlap significantly with other, sometimes treatable, conditions. There are many causes of memory loss, and the job of a neurology evaluation is to uncover the actual reason behind the symptoms — not simply assume the worst. Common Causes We Evaluate Possible Cause Typical Symptoms Is It Treatable? Alzheimer’s disease Gradual memory loss, confusion, language difficulty Manageable, not curable Mild Cognitive Impairment (MCI) Noticeable memory changes, daily function mostly intact Sometimes reversible Vitamin B12/folate deficiency Fatigue, confusion, memory lapses Yes, often fully treatable Thyroid disorders Brain fog, mood changes, slowed thinking Yes, with medication Depression & anxiety Forgetfulness, poor concentration, low motivation Yes Sleep disorders (including apnea) Daytime confusion, poor recall Yes Medication side effects Sudden onset confusion or memory issues Yes, often reversible Mini-strokes (TIAs) or vascular dementia Sudden memory gaps, focal weakness Partially manageable Past concussion or head injury Memory and concentration issues Varies by severity Finding the cause early makes treatment far more effective, whether that means correcting a vitamin deficiency or beginning a long-term care plan for Alzheimer’s disease. For more on how vascular health intersects with memory, see our post on Understanding TIAs and Mini-Strokes. Why Early Diagnosis Matters Catching Alzheimer’s disease early symptoms sooner rather than later changes the entire trajectory of care. Early action means: Better symptom control through targeted treatment Slower cognitive decline in many cases Safer daily functioning and reduced fall or wandering risk More time to plan and prepare legally, financially, and emotionally More effective medications, since several Alzheimer’s treatments work best in earlier stages Stronger support for caregivers and family members, who often carry the heaviest emotional load Waiting, on the other hand, often means more rapid decline and fewer treatment options by the time symptoms are addressed. If a loved one has recently been diagnosed, our guide on Supporting a Family Member With a New Diagnosis offers practical next steps for caregivers. Why Families Trust Consultant Corner Consultant Corner provides comprehensive, compassionate, expert care for memory loss and Alzheimer’s disease early symptoms, built around a thorough and personalized process. Full Neurology Evaluation A detailed review of symptoms, medications, mood, sleep, and risk factors gives our team a complete picture before any conclusions are drawn. Cognitive Testing Quick, effective in-office testing helps pinpoint both the type and severity of memory changes, distinguishing normal aging from something that needs closer attention. Review of CT/MRI Brain Scans When imaging is available or needed, we explain the changes clearly and identify signs consistent with Alzheimer’s disease, prior strokes, or other underlying causes. Personalized Treatment & Care Plan Every plan is built around the individual, combining medications, lifestyle changes, memory strategies, and safety guidance for the home. Support for Families & Caregivers Education, resources, and step-by-step recommendations help families feel less alone in the process. Same-Week Appointments Because memory concerns
Migraines: Common Triggers, Symptoms and Prevention Tips

Migraines: Common Triggers, Symptoms and Prevention Tips Migraine triggers are different for everyone, but almost every person who lives with migraines eventually learns that certain foods, habits, or environmental changes seem to set off an attack. If you have ever wondered why a stressful week, a skipped meal, or a glass of red wine left you in bed with a throbbing headache, you are not imagining it. Migraines are a real neurological condition, and understanding your personal migraine triggers is one of the most powerful steps you can take toward fewer, milder attacks. In the United States, migraines affect people of nearly every age group, though they are most common among adults between 18 and 44, and women are affected roughly three times more often than men. Severity tends to vary based on overall health, hormonal status, stress levels, and underlying conditions such as high blood pressure or sleep disorders. This guide walks through what migraines are, the most common migraine triggers, the symptoms that signal an attack is coming, and prevention strategies that actually work. What Is a Migraine, Exactly? A migraine is not “just a bad headache.” It is a neurological event that typically causes moderate to severe, pulsating pain, often on one side of the head. Migraines frequently come with nausea, vomiting, and heightened sensitivity to light and sound. Some people also experience an “aura” — visual disturbances like flashing lights or blind spots — before the pain even begins. Migraines can last anywhere from a few hours to several days, and for many people they are disabling enough to disrupt work, school, and family life. If headaches are interfering with your quality of life, it is worth getting a proper evaluation. You can read more about how different headache types are diagnosed in our related post, Tension Headaches vs. Migraines: How to Tell the Difference. Migraines: Who Is Most Affected? Migraine prevalence and severity shift across the lifespan: Children and teens: Migraines can begin as early as childhood, though they often present differently, with shorter attacks and more stomach-related symptoms. Adults 18–44: This is the peak age range for migraine frequency, often tied to work stress, hormonal cycles, and lifestyle factors. Women during reproductive years: Hormonal fluctuations make this group especially prone to migraines, particularly around menstruation. Adults over 50: Migraine frequency often declines with age, but severity and the risk of related health complications, like cardiovascular issues, can increase. Underlying health conditions also play a major role in severity. People managing high blood pressure, chronic stress, sleep apnea, or hormonal imbalances tend to experience more frequent and more intense migraine attacks. Common Migraine Triggers Identifying your personal migraine triggers is one of the most effective tools for prevention. While triggers vary from person to person, research and clinical experience point to several categories that affect most migraine sufferers. Dietary Migraine Triggers Aged cheeses and processed meats containing tyramine Alcohol, especially red wine Caffeine — both excessive intake and sudden withdrawal Artificial sweeteners and MSG Skipped meals or prolonged fasting Environmental and Sensory Triggers Bright or flickering lights Strong smells, including perfume, smoke, or cleaning products Sudden weather changes or barometric pressure shifts Loud noises or crowded environments Lifestyle and Physical Triggers Chronic stress or sudden emotional shifts (even relief after stress can trigger an attack) Poor sleep quality or irregular sleep schedules Dehydration Intense physical exertion Hormonal changes, particularly drops in estrogen during the menstrual cycle Why Tracking Triggers Matters Because migraine triggers are highly individual, keeping a simple headache diary — noting food, sleep, stress levels, and weather — can reveal patterns that are easy to miss otherwise. Many patients are surprised to discover that their attacks cluster around a specific combination of factors rather than a single cause. Recognizing Migraine Symptoms Early Migraines often unfold in four distinct phases, and recognizing early symptoms can help you intervene before the pain becomes severe. Phase Typical Symptoms Duration Prodrome Mood changes, food cravings, neck stiffness, fatigue Hours to 1–2 days before Aura (in some people) Visual flashes, blind spots, tingling sensations 5–60 minutes Attack Throbbing pain, nausea, light/sound sensitivity 4–72 hours Postdrome Exhaustion, difficulty concentrating, mild residual pain Up to 24 hours after Not everyone experiences all four phases, and aura occurs in only about a quarter of migraine cases. Still, learning to recognize your own prodrome symptoms can give you a valuable window to act — whether that means taking medication, resting in a dark room, or simply removing yourself from a triggering environment. If your headaches are accompanied by confusion, vision loss, severe sudden onset (“the worst headache of your life”), fever, neck stiffness, or symptoms following a head injury, seek emergency medical care immediately. These can indicate a more serious underlying issue that needs urgent attention. Migraine Prevention Tips That Actually Work Prevention is rarely about a single fix — it is about consistency across several areas of daily life. Stick to a regular sleep schedule. Going to bed and waking up at the same time every day, including weekends, helps stabilize the nervous system. Stay hydrated. Dehydration is one of the most overlooked migraine triggers, and something as simple as drinking water consistently throughout the day can reduce frequency. Eat at regular intervals. Skipping meals causes blood sugar swings that can provoke an attack. Limit known dietary triggers. Once you identify your personal food triggers through a headache diary, reducing or eliminating them can make a noticeable difference. Manage stress proactively. Techniques such as deep breathing, gentle exercise, and mindfulness can lower the frequency of stress-related migraines. Moderate caffeine and alcohol intake. Consistency matters more than total elimination for many people. Consider preventive medication or supplements. For people with frequent or severe migraines, a healthcare provider may recommend daily preventive treatment, magnesium, riboflavin, or other evidence-based options. Protect your eyes from screen strain. Frequent breaks and blue-light filtering can reduce visually triggered migraines, especially for people who spend long hours at a computer. For more on this, see our post
Ischemic Stroke: Early Warning Signs, Treatment and Recovery
Ischemic Stroke: Early Warning Signs, Treatment and Recovery Ischemic stroke is one of the most time-sensitive medical emergencies a person can face, and recognizing it within seconds can be the difference between full recovery and permanent disability. An ischemic stroke occurs when a blood vessel supplying the brain becomes blocked by a clot, cutting off oxygen and nutrients to brain tissue. Within minutes, brain cells begin to die, which is why doctors often say “time is brain.” Understanding the early warning signs, available treatments, and what recovery actually looks like can help you or a loved one act fast and get the right care when it matters most. In the United States, stroke remains one of the leading causes of death and long-term disability, and ischemic stroke accounts for the vast majority of all stroke cases. This disease is more common in certain age groups — particularly adults over 55 — but it can strike younger people too, especially those with uncontrolled blood pressure, diabetes, or heart conditions. Its severity often depends heavily on the underlying health of the individual, how quickly symptoms are recognized, and how fast appropriate treatment begins. This guide walks through everything you need to know about ischemic stroke: how to spot it early, why immediate evaluation saves lives, who is most at risk, what treatment looks like, and how recovery unfolds. If you’re looking for related reading, you may also want to check out our posts on Understanding TIA: The Warning Stroke You Shouldn’t Ignore and Managing High Blood Pressure to Protect Your Brain. What Is an Ischemic Stroke? An ischemic stroke happens when a blood clot or fatty deposit blocks an artery that carries blood to the brain. Roughly 87% of all strokes are ischemic, according to the American Stroke Association. Unlike a hemorrhagic stroke, which involves bleeding in the brain, an ischemic stroke is caused by an obstruction that starves brain tissue of oxygen-rich blood. The longer that blockage persists, the more brain cells die — which is why rapid diagnosis and treatment are critical. There are two primary types of ischemic stroke: Thrombotic stroke — a clot forms directly inside an artery in the brain, often where the artery has narrowed due to plaque buildup (atherosclerosis). Embolic stroke — a clot forms elsewhere in the body (often the heart) and travels through the bloodstream until it lodges in a brain artery. Both types produce similar symptoms and require emergency evaluation. Why Ischemic Stroke Is a True Medical Emergency Every minute an ischemic stroke goes untreated, the brain loses an estimated 1.9 million neurons. That’s why emergency departments and stroke centers are built around speed — every test, every decision, and every treatment window is measured in minutes, not hours. Recognize the Warning Signs Early Ischemic strokes strike suddenly, often without warning. If you notice any of these symptoms — even if they come and go — get emergency help immediately: Sudden weakness or numbness on one side of the face, arm, or leg Trouble speaking or understanding words Sudden vision loss or blurriness Dizziness, imbalance, or sudden trouble walking Intense, sudden headache with no known cause Use the FAST Test The FAST acronym is the simplest way to remember the warning signs of stroke: F — Face drooping A — Arm weakness S — Speech difficulty T — Time to call 911 These symptoms are your body’s alarm system. They are not something to “wait out” or sleep off — every ischemic stroke symptom deserves an immediate call to emergency services. Why Immediate Stroke Evaluation Saves Lives Acting quickly after stroke symptoms appear can determine whether a patient is eligible for time-sensitive treatments, including: Clot-busting medication (tPA), which must typically be given within 3 to 4.5 hours of symptom onset Mechanical clot removal (thrombectomy), which can be effective for certain large-vessel blockages within a longer window Advanced stroke prevention therapy to reduce the risk of a second event Even brief, fleeting symptoms can represent a TIA (transient ischemic attack), sometimes called a “mini-stroke.” A TIA is often the final warning sign before a major ischemic stroke, and it should never be ignored simply because symptoms resolved on their own. A fast evaluation after a TIA can prevent a far more serious, disabling stroke down the line. Treatment Window Intervention Best Candidate 0–4.5 hours from onset tPA (clot-busting medication) Confirmed ischemic stroke, no bleeding risk Up to 24 hours (select cases) Mechanical thrombectomy Large-vessel blockage confirmed on imaging Ongoing Blood pressure & cholesterol management All ischemic stroke and TIA patients Ongoing Antiplatelet or anticoagulant therapy Patients with clotting risk or atrial fibrillation Long-term Rehabilitation (physical, speech, occupational) Patients with post-stroke deficits Are You at Risk for an Ischemic Stroke? Some risk factors for ischemic stroke can be managed, while others cannot. Knowing your personal risk profile is one of the most powerful tools for prevention. Common risk factors include: High blood pressure (the No. 1 cause of stroke) Diabetes High cholesterol Atrial fibrillation or other heart disease Smoking or vaping Obesity and a sedentary lifestyle Previous stroke or TIA Family history of stroke According to the Centers for Disease Control and Prevention, nearly 80% of strokes are preventable through management of these risk factors. If you have one or more of these conditions, scheduling an early neurology consultation truly matters — prevention is almost always more effective, and less costly, than treating a stroke after it happens. You might also find it helpful to read our related article on How Atrial Fibrillation Increases Stroke Risk for a deeper look at the heart-brain connection. How Ischemic Stroke Is Diagnosed When someone arrives at the hospital with suspected stroke symptoms, doctors move quickly through a standardized evaluation process. This typically includes: A rapid neurological exam to assess speech, vision, strength, and coordination CT or MRI imaging of the brain to confirm whether the stroke is ischemic or hemorrhagic Blood tests to check clotting factors, glucose, and other markers Imaging of the blood vessels (CT
Head Injury Explained: Symptoms, Recovery and Medical Care

Head Injury Explained: Symptoms, Recovery and Medical Care A head injury can happen in the blink of an eye — a bathroom fall, a collision on the road, a sports impact, or even an accidental knock against a cabinet door. But the effects can ripple outward through days, weeks, or even months of your life. Understanding what a head injury actually means, knowing which symptoms signal danger, learning what recovery really looks like, and recognizing when to call a doctor can make a profound difference in how fully — and how quickly — you or someone you love recovers. This comprehensive guide covers everything you need to know about head injury: the different types, the common and emergency warning signs, the full stages of recovery, the special populations most at risk, how doctors make a diagnosis, and the practical steps you can take right now to protect your brain health. What Is a Head Injury? A head injury is any form of trauma to the scalp, skull, or brain. The spectrum is wide — ranging from a minor bump that leaves a small lump and fades within a day, all the way to a traumatic brain injury (TBI) that disrupts memory, mood, movement, or consciousness for months or longer. Not every head injury directly involves the brain. A scalp laceration may bleed dramatically because scalp tissue is highly vascular, yet involve zero brain trauma. Conversely, a head injury that appears minor on the surface can still cause significant internal damage to the brain beneath the skull. Medically, head injuries fall into two primary categories: Closed Head Injuries The skull remains intact, but the brain can still be jolted, bruised, or twisted inside the cranial cavity. The most common type is a concussion, which occurs when the brain moves rapidly within the skull and temporarily disrupts normal brain function. Closed head injuries account for roughly 75% of all traumatic brain injuries in the United States each year. Open (Penetrating) Head Injuries An object breaches the skull and may directly damage brain tissue. These are generally more severe, almost always require emergency surgical intervention, and carry a significantly higher risk of permanent neurological damage. Within both categories, a head injury is further classified by severity — mild, moderate, or severe — based on whether the person lost consciousness, how long confusion lasted, and what brain imaging reveals. How Common Is Head Injury? Head injury is far more common than most people realize. According to the Centers for Disease Control and Prevention (CDC), approximately 1.7 million traumatic brain injuries occur in the United States each year, with about 3% resulting in death. Adults are the most frequently affected group, though children and older adults face their own heightened risks that deserve special attention. Common Causes of Head Injury The cause of a head injury often shapes the type and severity of the damage that follows. Understanding the mechanism matters, because high-energy impacts — such as those in motor vehicle accidents or falls from height — carry a much higher likelihood of serious brain injury even when initial symptoms appear mild. The most common causes include: Falls — Falls are the single leading cause of head injury overall, particularly in young children and adults over age 65. Poor balance, vision changes, and medications that impair coordination all significantly elevate fall risk in older adults. Motor Vehicle Accidents — The forces involved in car collisions tend to produce more severe injuries. Whiplash-type movements can cause the brain to strike the interior of the skull even when there is no direct head impact. Sports-Related Impacts — Contact sports like football, soccer, rugby, hockey, and boxing frequently produce concussions. Even cycling and skiing carry significant head injury risk without a properly fitted helmet. Workplace Accidents — Construction and industrial workers face elevated risk from falling objects, falls from elevated platforms, or machinery-related impacts. Physical Assaults — Blunt force trauma to the head during an assault accounts for a meaningful percentage of emergency department head injury visits each year. Head Injury Symptoms: What to Watch For One of the most critical things to understand about a head injury is that symptoms do not always appear immediately. They can emerge hours — sometimes even a day or two — after the initial trauma. This delayed onset is precisely why anyone who sustains a head injury should be monitored closely for at least 24 to 48 hours, even when they feel completely fine right after the incident. Common Symptoms of a Head Injury Persistent or worsening headache Dizziness or problems with balance and coordination Nausea or vomiting Confusion, mental fog, or difficulty concentrating Memory problems, especially difficulty recalling the injury event itself (post-traumatic amnesia) Sensitivity to light (photophobia) or noise (phonophobia) Unusual fatigue or drowsiness Irritability, mood swings, or heightened anxiety Ringing in the ears (tinnitus) or blurred vision Disrupted sleep — either difficulty falling asleep or sleeping far more than usual These symptoms overlap considerably with other neurological conditions. For instance, a persistent headache after a head injury can look very similar to a migraine disorder. If you’ve been experiencing recurrent headaches, our related guide — Can Bad Posture Cause Headaches? Causes, Symptoms & Treatment — explores how different structural triggers can produce overlapping symptoms. Emergency Warning Signs After a Head Injury While many head injury symptoms can be managed with rest and careful at-home monitoring, certain signs demand immediate emergency care. Brain swelling and internal bleeding can develop without any visible external injury, and these are conditions that can become life-threatening very rapidly. Call 911 or Go to the Emergency Room Immediately If: The headache rapidly intensifies rather than easing There is repeated or forceful vomiting (more than once or twice) The person has slurred speech or sudden difficulty finding words A seizure or convulsion occurs One pupil is noticeably larger than the other (unequal pupils) The person shows growing confusion, extreme disorientation, or dramatic behavioral change There is any loss of consciousness, even briefly
Post-Stroke Recovery & Rehabilitation

How the Brain Heals and What Truly Drives Recovery A Neurologist-Guided, Patient-Centered Roadmap Stroke Recovery Is a Neurological Process — Not a Waiting Period A stroke is not simply a sudden medical event; it is a neurological injury that disrupts the brain’s ability to control movement, speech, cognition, behavior, and vital bodily functions. Whether caused by an ischemic blockage or an intracerebral hemorrhage, stroke results in acute damage to brain tissue followed by a complex and evolving recovery process. In the United States, nearly 800,000 people experience a stroke each year, making it one of the leading causes of long-term neurological disability. Advances in acute stroke treatment have significantly improved survival. However, survival is only the beginning. What follows is a prolonged and highly individualized process of neurological recovery. For patients and families, this phase is often filled with uncertainty:Will strength return? Will speech improve? How long does recovery take? Is rehabilitation truly effective? From a neurological standpoint, recovery is best understood through two core principles: Stroke recovery is driven by brain plasticity, not time alone Rehabilitation is an active neurological treatment, not supportive care Understanding these principles helps patients and caregivers move forward with clarity, realistic expectations, and hope. How the Brain Heals After Stroke: Understanding Neuroplasticity When a stroke occurs, part of the brain is injured or deprived of blood flow, leading to loss of neurons and disruption of neural networks. Importantly, this injury does not mean the brain is incapable of recovery. Instead, recovery depends on how surviving brain regions adapt over time — a process known as neuroplasticity. What Is Neuroplasticity? Neuroplasticity refers to the brain’s ability to reorganize, strengthen existing connections, and form new neural pathways in response to injury and experience. After a stroke, unaffected areas of the brain can partially assume functions previously handled by damaged regions. This biological adaptability is the foundation of rehabilitation. Crucially, neuroplasticity is activity-dependent. The brain does not reorganize simply with rest or time. Recovery is driven by repetitive, meaningful, task-specific practice, which is why structured rehabilitation is so effective. Early and Late Brain Recovery In the first days to weeks after a stroke, the brain enters a period of heightened plasticity. Swelling subsides, inflammation decreases, and neural signaling stabilizes. During this phase, early improvements may reflect recovery of stunned but viable tissue. While the most rapid gains often occur within the first 3–6 months, recovery does not stop there. Research shows that meaningful improvement can continue for 6–12 months and beyond, particularly when rehabilitation remains progressive and goal-directed. Later recovery often involves: Refinement of motor control rather than large strength gains Improved balance, coordination, and endurance Gradual improvements in language and cognition Development of compensatory strategies that enhance independence The idea that recovery “plateaus” early is often a reflection of reduced therapy intensity or lack of reassessment — not a true limit of neurological potential. Rehabilitation Therapies That Drive Recovery Stroke rehabilitation is not a single therapy or a one-size-fits-all program. It is a multidisciplinary neurological intervention designed to retrain the brain by engaging impaired neural networks repeatedly and purposefully. Physical Therapy: Restoring Mobility and Balance Physical therapy focuses on improving strength, coordination, balance, and gait. Weakness, spasticity, and impaired balance are common after a stroke and significantly affect independence. Through task-oriented and repetitive movement training, physical therapy helps the brain re-map motor pathways, reduce fall risk, and improve functional mobility. Therapy evolves — from basic transfers to higher-level balance, endurance, and community mobility. Occupational Therapy: Regaining Independence in Daily Life Occupational therapy helps patients regain the ability to perform activities of daily living, such as dressing, bathing, eating, writing, and managing household tasks. Stroke often affects fine motor control, visual-spatial processing, and executive function — all critical for daily independence. OT integrates motor, sensory, and cognitive systems, reinforcing purposeful use of affected limbs and promoting functional recovery rather than learned non-use. Speech and Language Therapy: Communication and Swallowing Stroke can affect language (aphasia), speech clarity (dysarthria), cognition, and swallowing (dysphagia). Speech-language therapy addresses: Language comprehension and expression Speech articulation and voice control Cognitive-communication skills Swallowing safety and nutrition Recovery in this domain may be gradual, but meaningful gains can continue long after motor recovery stabilizes. Early swallowing evaluation is essential to reduce aspiration risk and medical complications. Cognitive Rehabilitation: Attention, Memory, and Executive Function Cognitive changes after stroke are common and frequently underrecognized. Patients may struggle with attention, memory, processing speed, or executive skills — even when physical recovery appears strong. Cognitive rehabilitation helps patients develop new strategies to strengthen preserved neural pathways and compensate for deficits. Recovery in this domain often continues later into the recovery process, reinforcing the importance of ongoing reassessment. Early Recovery: The First Weeks Matter — But Don’t Define Everything The first days to weeks after a stroke represent a critical window of opportunity. During this phase, early mobilization and rehabilitation — when medically appropriate — improve functional outcomes and reduce complications. That said, early appearance does not define long-term outcome. Neurologists caution against premature prognostication. Patients may appear severely impaired early on yet make meaningful gains over time, while others with milder strokes may struggle due to secondary complications. Common early challenges include: Fatigue Fluctuating weakness or tone Speech or swallowing difficulty Cognitive slowing or confusion Emotional distress These challenges are common and treatable. Addressing them early improves participation in rehabilitation and long-term outcomes. What Really Predicts Stroke Recovery Recovery is shaped by multiple interacting factors — not a single variable. What Matters Most: Quality, timing, and intensity of rehabilitation Patient engagement and education Ongoing neurological oversight Social and caregiver support Management of medical and neurological complications What Matters Less Than Commonly Believed: Age alone (older adults retain neuroplastic capacity) Early severity as a fixed predictor Arbitrary recovery timelines From a neurologist’s perspective, trajectory over time is far more meaningful than a single snapshot. Cognitive, Emotional, and Behavioral Recovery Physical recovery is often the most visible aspect of stroke rehabilitation, but cognitive and emotional changes can be equally impactful. Cognitive Changes Difficulties with attention, memory, executive function, or visual-spatial processing may affect independence, work, and social engagement. These deficits may emerge
7 Subtle Stroke Signs in Women You Might Be Missing
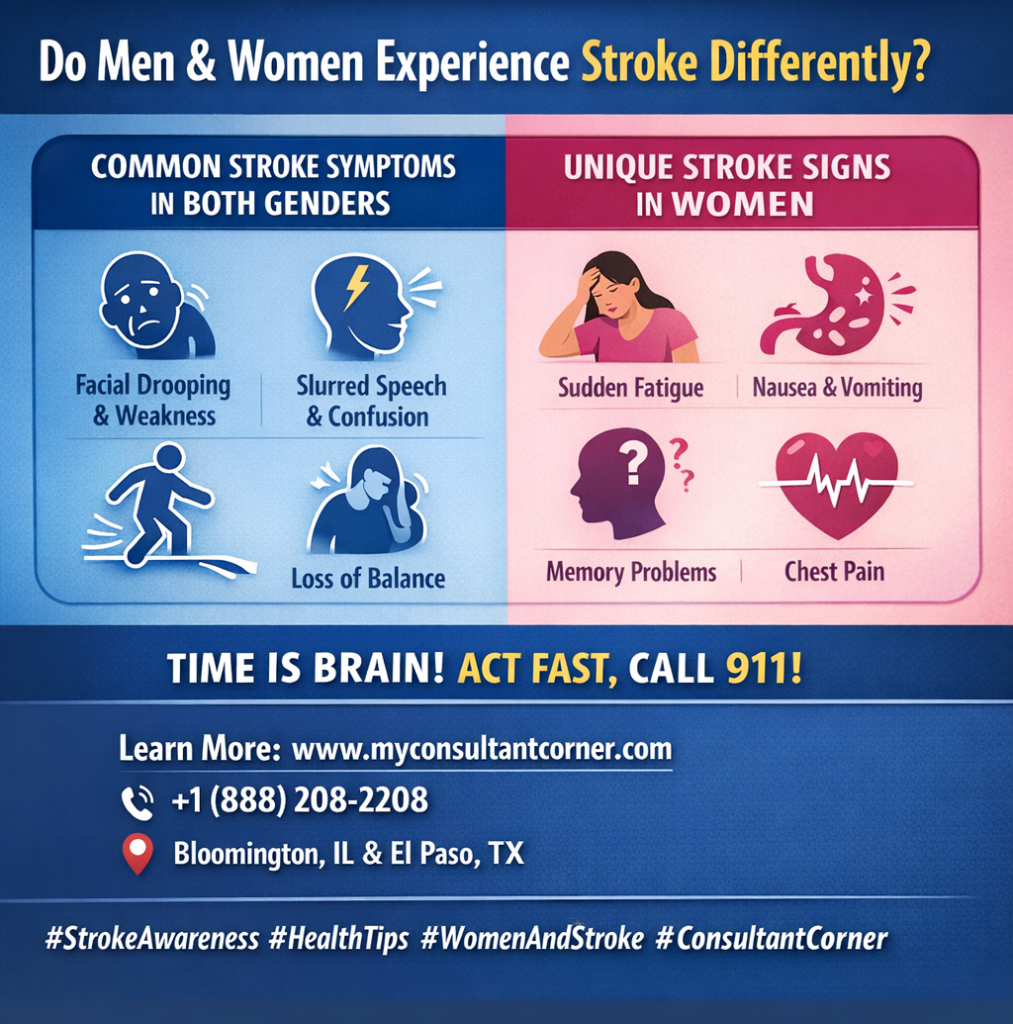
Do Men and Women Experience Stroke Differently? While the core mechanics of a stroke remain the same, clinical data show significant differences in how symptoms manifest based on gender. According to the World Stroke Organization (WSO), women are not only more likely to experience a stroke in their lifetime. Still, they are also 11% more likely to report non-traditional symptoms that lead to delayed diagnosis. Understanding these nuances is vital because every 60 seconds of delayed treatment results in the death of nearly 2 million brain cells. What Common Symptoms Are Shared by Both Genders? In the majority of cases, both men and women will display the “classic” neurological deficits associated with brain cell death. These symptoms are primarily focused on motor skills and sensory processing: Sudden Asymmetry: Drooping of the face, or paralysis of the arm or leg—typically isolated to one side of the body. Cognitive & Sensory Disruptions: Slurred speech, sudden confusion, vision loss, or a severe headache with no identifiable cause. Mobility Issues: Difficulty walking or a sudden loss of balance (the “B” in the BE FAST protocol). Why Are Stroke Signs Frequently Missed in Women? Women are more likely to present with “subtle” or nonspecific symptoms, which are often mistakenly attributed to stress, exhaustion, or other minor ailments. This diagnostic gap is a leading cause of poorer outcomes for female patients. Common “Non-Traditional” Symptoms in Women: Systemic Weakness: A feeling of generalized exhaustion or extreme fatigue that comes on suddenly. Gastrointestinal & Respiratory Signs: Nausea, vomiting, hiccups, or shortness of breath. Altered Mental Status: Disorientation, sudden memory problems, or acting “out of character”. Cardiac Mimics: Chest pain, palpitations, or a racing heartbeat that can sometimes be confused with a heart attack. Which Symptoms Are Relatively More Common in Men? Research suggests men are more likely to exhibit specific coordination and sensory issues. While these are still “classic” signs, they appear with higher frequency in male patients: Ataxia: A sudden, noticeable loss of coordination in the limbs or an unsteady gait. Paresthesia: Distinct sensations of numbness, tingling, or “pins and needles”. Visual Disturbances: Higher reported rates of double vision or sudden dimming of sight in one eye. How Does Gender Affect Treatment Timing and Survival? Feature Statistical Impact on Women Impact on Recovery Recognition Nonspecific signs (nausea, fatigue) lead to frequent misdiagnosis. Delayed treatment. Response Time Women wait an average of 30 to 60 minutes longer to call 911. Increased brain damage. Age of Onset Women typically have strokes at an older age than men. Higher risk of mortality. Disability Risk Women face a higher rate of long-term nursing home placement post-stroke. Reduced independence. When Should You Seek Emergency Help? Regardless of sex, any sudden combination of these symptoms—even if they seem mild or resolve after a few minutes—must be treated as a medical emergency. Call Emergency Services (911): Do not wait for a clinic appointment or try to “sleep it off”. Trust Your Instincts: If a woman reports feeling “not right” combined with sudden fatigue or confusion, seek help immediately. Time is Brain: Accessing clot-busting therapies within the first 3–4.5 hours is the most effective way to prevent permanent disability. Your Recovery Doesn’t End at the Hospital Doors At Consultant Corner, we believe that surviving a stroke is only the beginning. We treat stroke recovery as a continuous journey, not a one-time medical event. Our specialized neurology team offers personalized, data-driven post-stroke care through both convenient virtual consultations and in-person clinic visits. We focus on neuroplasticity, secondary prevention, and restoring your independence. Take the Next Step Toward Healing If you or a loved one needs expert guidance on the path to recovery, our team is ready to support you. Visit: www.myconsultantcorner.com Call: +1 (888) 208-2208 Email: info@myconsultantcorner.com Address: 1404 Eastland Dr, Bloomington, IL 61701, United States Address: 5140 Montana Ave, El Paso, TX 79903, United States
5 Early Stroke Symptoms You Can’t Ignore (2026 Update)
What Are the Main Warning Signs of a Stroke? A stroke happens when blood flow to a part of the brain is interrupted, leading to brain cell damage within minutes. Recognizing the early warning signs can save your life or someone else’s. According to the World Health Organization (WHO), stroke is the second leading cause of death globally, responsible for over 12 million cases every year. Time is critical—knowing the signs and acting fast can reduce the risk of long-term disability and improve recovery outcomes. How Can You Identify Stroke Symptoms Quickly? (Remember: BE FAST) Medical experts use the BE FAST acronym to help people quickly recognize stroke symptoms. Each letter stands for a potential warning sign: B – Balance: Is There Sudden Dizziness or Loss of Coordination? If someone suddenly can’t walk straight, feels dizzy, or loses coordination, it could be an early stroke sign. Research from the American Stroke Association (ASA) suggests that around 40% of stroke patients experience balance problems or sudden dizziness. E – Eyes: Is There Trouble Seeing Clearly? Watch for blurred vision, double vision, or complete vision loss in one or both eyes. About 20% of stroke victims report sudden vision changes, which may appear alongside light sensitivity or visual field loss. F – Face: Is One Side Drooping? Ask the person to smile. If one side droops or feels numb, it’s a red flag. Facial asymmetry is one of the most common early signs of stroke and appears in over 60% of cases according to clinical data. A – Arm: Do the Arms Feel Weak or Numb? Have them raise both arms. If one arm drifts downward or can’t be lifted, that’s a strong indicator of a stroke. This weakness may also affect one leg, typically on the same side. S – Speech: Is the Speech Slurred or Confusing? Speech problems—like slurred words, difficulty understanding, or trouble finding the right words—often signal a stroke. Studies find that nearly 70% of stroke patients present some form of speech impairment at onset. T – Time: Why Is Every Minute Critical? If any of these signs appear, call emergency services immediately. Never wait for the symptoms to improve on their own. Each passing minute can cause an estimated 1.9 million brain cells to die, increasing the risk of permanent brain injury. What Are Other Sudden Symptoms Not to Ignore? Not every stroke follows the same pattern. Some people experience less common, but equally serious symptoms such as: Sudden, severe headache without a known cause—especially if it comes out of nowhere. Loss of consciousness, fainting, or seizure. Nausea, vomiting, or vertigo (a spinning sensation). Sudden confusion or trouble understanding speech. Always treat these as potential emergencies—even if symptoms fade after a few minutes. Why Is Early Recognition of Stroke So Important? When it comes to stroke, every minute truly counts. Each second of delay means more brain cells are lost, and long-term complications become more likely. The World Health Organization (WHO) reports that strokes cause over 6.5 million deaths globally each year, and the risk of severe disability rises sharply with every lost minute of treatment time. In short, the faster a stroke is recognized and treated, the better the outcome. Why Does Fast Action Improve Access to Treatments? Stroke treatments are highly time-sensitive. Clot-busting drugs (known as thrombolytics, such as tPA) and mechanical clot removal procedures must be given within 3 to 6 hours from symptom onset to be most effective. When strokes are recognized quickly: Patients reach CT scans faster, helping doctors confirm the stroke type (ischemic or hemorrhagic). Life-saving therapies can be started sooner, limiting brain damage. Supportive care (like managing blood pressure, oxygen, and glucose) can prevent secondary complications such as brain swelling or infection. In contrast, delayed recognition may mean missing the treatment window entirely, reducing the chance of recovery. How Does Early Recognition Improve Survival and Recovery? Evidence is clear: faster diagnosis leads to better survival and long-term independence. A large-scale study in The Lancet Neurology found that patients treated within the first 90 minutes of a stroke were three times more likely to recover without major disability. Prompt recognition and treatment also mean: Lower mortality rates. Fewer hospital complications, such as blood clots and pneumonia. Greater chances of walking and speaking normally after recovery. Essentially, time to treatment predicts quality of life after stroke. When Should You Go to the ER for a Stroke? If you suspect a stroke—even slightly—call emergency services immediately. Don’t wait to see if symptoms improve, and don’t try to drive yourself. Stroke is a time‑critical medical emergency, and fast action can mean the difference between full recovery and permanent disability. According to the American Heart Association, early treatment within the first few hours can reduce disability by up to 30% and significantly improve survival. The Consultant Corner Approach to Ischemic Stroke At Consultant Corner, we view ischemic stroke as an ongoing recovery process, not a single event. Our neurology team provides personalized post-stroke care through both in-clinic and virtual visits, focusing on recovery, prevention, and long-term brain health. Take the Next Step If you or a loved one is recovering from an ischemic stroke, we’re here to help.Visit www.myconsultantcorner.com, call: +1 (888) 208-2208, or Email: info@myconsultantcorner.com to get started. Address: 1404 Eastland Dr, Bloomington, IL 61701, United States Address: 5140 Montana Ave, El Paso, TX 79903, United States