Migraine and Temporomandibular Disorders - What Is the Connection and Why Does It Matter?

Your ears feel full, and your neck is tense. You have tried pain relief, but nothing seems to fully work – because no one has connected the dots yet.
Migraines and temporomandibular disorders are two of the most commonly misdiagnosed conditions in neurology and dental medicine. Individually, each one is challenging enough to manage. Together, they create a cycle of overlapping pain that is difficult to break without understanding how they are connected.
This article explains the relationship between migraine and TMJ disorder, why one condition can trigger or worsen the other, and what effective treatment looks like when both are present.
What Is Temporomandibular Disorder (TMD)?
Temporomandibular disorder – also called TMD or TMJ disorder – refers to a group of conditions affecting the temporomandibular joint, the surrounding muscles, and the associated nerves and tissues.
The temporomandibular joint is the hinge that connects your lower jaw to your skull, located just in front of each ear. It is one of the most used joints in the body – active every time you chew, speak, yawn, or swallow.
When this joint becomes inflamed, misaligned, or placed under excessive stress, it produces a range of painful symptoms that can extend well beyond the jaw.
Common causes of TMJ disorder include:
- Bruxism – chronic teeth grinding, most often during sleep
- Jaw clenching – frequently driven by stress or anxiety
- Bite misalignment (malocclusion)
- Previous jaw injury or trauma
- Arthritis of the temporomandibular joint
- Sleep apnea, which has a documented connection to jaw muscle overactivity
- Postural problems – particularly forward head posture
TMD affects an estimated 10 to 15 percent of adults, with women between the ages of 20 and 40 being the most commonly affected group.
What is a migraine?
Family history remains one of the strongest indicators of migraine risk. Research consistently shows that migraines occur more
Migraine is a neurological disorder – not simply a severe headache. It involves complex changes in brain activity, nerve signaling, and blood flow that produce intense, recurring episodes of pain along with a distinctive set of associated symptoms.
A migraine attack typically passes through several phases:
- Prodrome – hours or days before the headache, patients may notice mood changes, fatigue, food cravings, or neck stiffness
- Aura – in about 30 percent of cases, visual disturbances, tingling, or speech changes occur just before the headache
- Headache phase – throbbing or pulsating pain, usually on one side, lasting 4 to 72 hours
- Postdrome – a recovery phase of fatigue, brain fog, or sensitivity that can last up to 24 hours after pain resolves
Chronic migraine is defined as 15 or more headache days per month for more than three months, with at least 8 of those days meeting migraine criteria. It is one of the leading causes of disability among neurological conditions
Persistent Headaches and Jaw Pain? Get Expert Neurological Guidance
The Connection Between Migraines and Temporomandibular Disorders
The relationship between migraine and temporomandibular disorders is well-established in the medical literature – yet it remains underrecognized in clinical practice.
Studies consistently show that people with TMJ disorder are significantly more likely to experience migraine than those without it. Research estimates the overlap ranges from 30 to 50 percent of patients with one condition also having features of the other.
This is not a coincidence. It reflects a shared biological mechanism.
The Trigeminal Nerve - Connection
The trigeminal nerve is the primary pain pathway connecting TMJ disorder and migraine.
This nerve – the largest cranial nerve – has three branches that spread across the forehead, cheek, jaw, and temples. It carries sensory information from the entire face and head to the brain.
In migraine: The trigeminal nerve becomes activated and releases inflammatory neuropeptides – particularly CGRP (calcitonin gene-related peptide) – that dilate blood vessels and generate the throbbing pain of a migraine attack.
In TMJ disorder, Mechanical stress, inflammation, or muscle tension in the jaw area directly irritates the trigeminal nerve branches that pass through that region.
When TMJ disorder is active, it keeps a low level of trigeminal nerve irritation running continuously in the background. For a person already predisposed to migraine, this ongoing irritation lowers the threshold needed to trigger a full migraine attack – making episodes more frequent, more severe, and harder to control.
Symptoms - How Migraine and TMJ Disorder Overlap

Understanding which symptoms belong to which condition – and where they overlap – is essential for accurate diagnosis.
Symptoms of TMJ Disorder
- Jaw pain or soreness – especially in the morning
- Clicking, popping, or grinding sounds from the jaw joint
- Difficulty or pain when opening the mouth wide
- Jaw locking – stuck open or closed
- Headaches concentrated around the temple and jaw
- Ear pain or a feeling of pressure in the ear – without infection
- Tinnitus – ringing, buzzing, or humming in the ears
- Dizziness or vertigo
- Facial pain – often described as aching or pressure
- Neck pain and shoulder tension
- Teeth showing abnormal wear patterns
Symptoms of Migraine
- Moderate to severe head pain – usually throbbing or pulsating
- Pain typically on one side of the head
- Nausea or vomiting
- Sensitivity to light – photophobia
- Sensitivity to sound – phonophobia
- Visual aura – zig-zag lines, flashing lights, or temporary blind spots
- Tingling or numbness in the face or hands
- Pain that worsens with physical activity
- Attacks lasting 4 to 72 hours
- Fatigue, brain fog, or mood changes before or after the headache
Symptoms That Appear in Both Conditions
- Temple pain and pressure
- Facial pain
- Neck pain and stiffness
- Ear pain or discomfort
- Dizziness
- Sleep disruption
- Pain triggered or worsened by stress
This overlap is precisely why both conditions are frequently misdiagnosed – and why many patients receive treatment for one while the other continues driving their symptoms.
Can TMJ Cause Migraines?
Yes – and the evidence for this is substantial.
TMJ disorder does not simply mimic migraine. In susceptible individuals, it can directly trigger migraine attacks through the following mechanisms:
- Sustained trigeminal nerve irritation. Chronic jaw muscle tension, joint inflammation, or joint dysfunction keeps the trigeminal nerve in a state of low-level activation. In a brain prone to migraine, this acts as a continuous trigger – eventually initiating a full migraine cascade.
- Muscle tension spreading to the head. The muscles of the jaw, temples, and neck are all interconnected. Tension in the masseter and temporalis muscles – which are directly involved in TMJ disorder – can radiate upward into the scalp and temples, initiating or worsening a migraine episode.
- Bruxism as a direct trigger. Teeth grinding generates significant force through the jaw and skull. The muscle fatigue and micro-trauma produced by nighttime bruxism can trigger morning headaches that meet the criteria for migraine attacks. Many patients with undiagnosed bruxism experience their worst migraines first thing in the morning.
- Sleep disruption TMJ disorder, particularly when associated with sleep bruxism or sleep apnea, severely disrupts sleep quality. Poor sleep is one of the most consistent and powerful migraine triggers. Patients who grind their teeth often wake repeatedly throughout the night without realizing it – and the resulting sleep deprivation directly increases migraine frequency.
- Stress as a shared amplifier. Stress worsens both conditions simultaneously. Psychological stress increases jaw clenching and bruxism, which inflames the TMJ and increases trigeminal irritation – and stress is also one of the most reliable migraine triggers. In patients with both conditions, a stressful period can cause both to flare simultaneously, making the combined pain particularly severe.
Does TMJ Make Migraines Worse?
Yes, particularly in patients with chronic migraine.
Even if TMJ disorder did not cause the migraines originally, its presence makes migraines significantly harder to manage. Patients with untreated TMJ disorder typically experience:
- Higher migraine frequency – more days per month with headache
- Greater migraine severity – attacks that are more intense and last longer
- Poorer response to migraine medications – because the underlying trigeminal irritation from the jaw is not being addressed
- Faster progression toward chronic migraine – the ongoing jaw-related trigeminal activation accelerates the sensitization process
In clinical practice, neurologists regularly see patients whose migraines were well-controlled for years – until a jaw injury, new stress-related bruxism, or dental changes introduced a TMJ component. Once that happens, previously effective migraine treatments may become insufficient on their own.
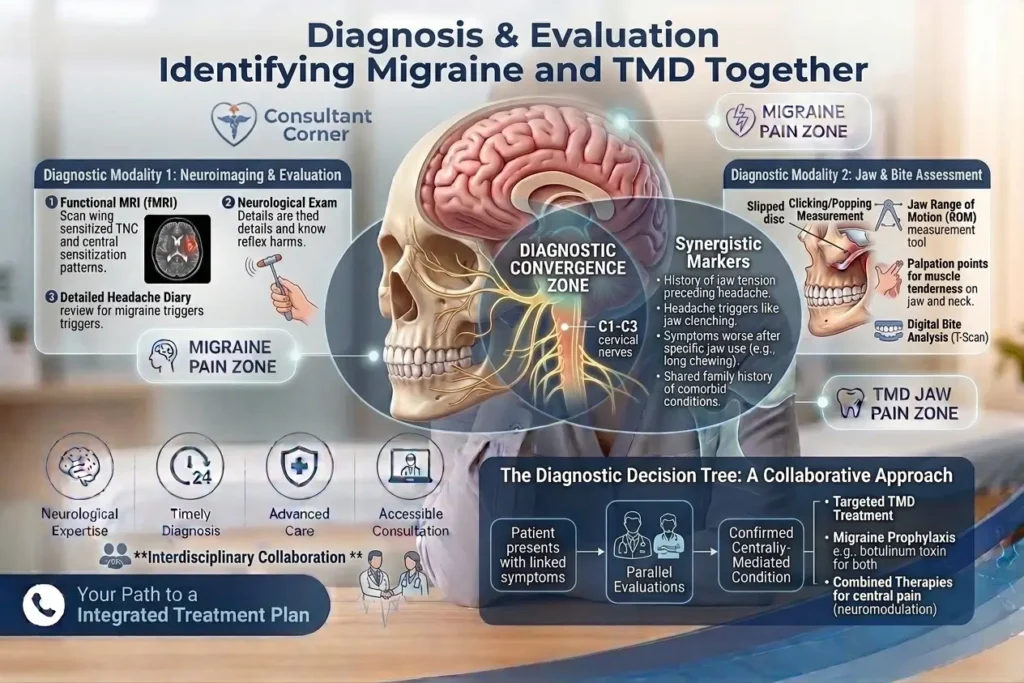
Diagnosis - How Are These Conditions Identified Together?
Accurate diagnosis of both migraine and temporomandibular disorder requires a thorough clinical evaluation – and ideally, coordination between a neurologist and a dental specialist.
Neurological Evaluation
A neurologist or headache specialist will assess:
- The character, location, duration, and frequency of headaches
- Associated symptoms – nausea, light sensitivity, aura, neck stiffness
- Migraine triggers and patterns
- Response to previous headache treatments
- Whether headache frequency meets criteria for chronic migraine
TMJ Assessment
A dentist or oral specialist will evaluate:
- Range of jaw motion and any restriction or pain on opening
- Joint sounds – clicking, popping, or crepitus
- Tenderness in the masseter, temporalis, and pterygoid muscles
- Signs of bruxism – worn tooth surfaces, jaw muscle hypertrophy
- Bite alignment
- Imaging – panoramic X-ray or MRI of the TMJ if needed
The Diagnostic Challenge
The primary challenge is that these specialties do not always communicate with each other. A patient may receive excellent migraine care from a neurologist while an unaddressed TMJ disorder continues triggering attacks. Or a dentist may fit a night guard for bruxism without recognizing that the patient also has a chronic migraine condition requiring separate neurological management.
If you have both jaw symptoms and frequent headaches, it is worth raising both with every provider you see – and seeking care from specialists who recognize the connection.
Treatment - Migraine and TMD Disorder Together
Effective treatment for overlapping migraine and temporomandibular disorder requires addressing both conditions simultaneously.
TMD Disorder Treatment
Oral appliance therapy: A custom-fitted night guard or oral splint reduces the impact of bruxism, repositions the jaw joint, and protects tooth surfaces. This is often the first-line treatment for TMJ disorder and can produce significant relief – including reduction in associated headaches.
Physical therapy: Targeted exercises and manual therapy for the jaw, neck, and shoulder muscles reduce muscle tension, improve joint mobility, and address postural factors that contribute to TMJ dysfunction.
Botox for jaw muscle tension: Botox injections into the masseter and temporalis muscles reduce the force of jaw clenching and grinding. This is particularly effective for patients whose TMJ disorder is driven primarily by muscle overactivity rather than structural joint problems.
Stress management Because stress drives both jaw clenching and migraine attacks, stress reduction strategies – including cognitive behavioral therapy, mindfulness, and sleep hygiene improvements – are a meaningful part of TMJ treatment.
Dietary adjustments. During active TMJ flares, a soft food diet reduces mechanical stress on the joint and allows inflammation to settle.
Migraine Treatment
Acute treatment: Medications taken at the onset of a migraine attack to stop it in its progress. These include triptans, gepants (CGRP receptor antagonists), and ditans. Early treatment – before pain becomes severe – produces the best outcomes.
Preventive treatment for patients with frequent or chronic migraine, daily preventive medication reduces attack frequency and severity. Options include:
- CGRP monoclonal antibodies – a targeted class of migraine preventives that block the CGRP pathway directly involved in migraine attacks
- Beta-blockers
- Antiepileptic medications
- Tricyclic antidepressants
Botox for chronic migraine Botox injections for chronic migraine – administered by a neurologist across specific head and neck sites – are FDA-approved and highly effective for patients with 15 or more headache days per month. This is distinct from Botox used for TMJ, though in patients with both conditions, treatment planning can sometimes be coordinated.
Trigger management: Identifying and addressing personal migraine triggers – including sleep disruption, dietary factors, hormonal fluctuations, and stress – reduces overall attack frequency.
When Both Are Treated Together
Research and clinical experience consistently show that patients who receive treatment for both conditions simultaneously achieve better outcomes than those treated for one alone.
In particular, treating the TMJ component can meaningfully reduce migraine frequency, sometimes allowing previously inadequate migraine treatments to become effective again, because the underlying trigeminal trigger has been reduced.
Who Should You See?
See a neurologist or headache specialist if:
- Headache is your dominant complaint – regardless of whether jaw symptoms are also present
- You have nausea, light or sound sensitivity, or visual symptoms with your headaches
- Your headaches occur 10 or more days per month
- Your migraine medications are not providing adequate relief
- You suspect both conditions may be present and want a coordinated evaluation
See a dentist or TMJ specialist if:
- Jaw clicking, locking, or limited mouth opening is your primary concern
- Pain is clearly triggered by jaw movement and relieved by jaw rest
- You have significant bruxism, and your headaches are relatively mild
For most patients with overlapping symptoms, starting with a neurologist is the right first step. A neurologist can evaluate the headache component, identify whether TMJ disorder is contributing, and coordinate referral to the appropriate dental specialist – ensuring both conditions are addressed as part of a single, coherent treatment plan.
In My Consultant Corner, our neurology team has experience evaluating patients with complex headache presentations – including those where migraine and temporomandibular disorder overlap. We offer both in-person and online neurology consultations, so patients can access expert headache evaluation on a schedule that works for them.
Final Thought
Migraines and temporomandibular disorders are not separate problems that happen to occur in the same person. In many patients, they are interconnected conditions that share a common nerve pathway, feed each other through shared triggers, and combine to create a burden of pain that neither condition alone fully explains.
Understanding this connection is the first step. Getting the right evaluation – one that considers both the neurological and the structural components of your pain – is what makes effective treatment possible.
If you are living with frequent headaches, jaw pain, or a combination of symptoms that have not been fully explained, a thorough neurological evaluation is the right place to start.
My Consultant Corner provides expert consultation for migraine, chronic headache, and related neurological conditions. Our team is available for in-person and online appointments to help you get clear answers and a treatment plan that addresses the full picture.
Frequently Asked Questions
What is the connection between migraine and temporomandibular disorders (TMD)?
Migraine and temporomandibular disorders are connected through the trigeminal nerve, the primary pain pathway in the face and head. TMJ dysfunction can irritate this nerve, increasing the likelihood of migraine attacks and making existing migraines more difficult to control.
Why do migraine and TMJ disorder often occur together?
These conditions share common pain pathways, triggers, and risk factors, including stress, sleep disturbances, muscle tension, and trigeminal nerve activation. As a result, many patients experience symptoms of both conditions simultaneously.
Can treating TMJ disorder help reduce migraine frequency?
Yes, For patients with both conditions, addressing TMJ dysfunction through oral appliances, physical therapy, stress management, or other treatments may reduce trigeminal nerve irritation and help decrease migraine frequency and severity.
How can I tell if my headaches are related to TMJ disorder? bleed after a fall?
Headaches linked to TMJ disorder often worsen with chewing, talking, yawning, or jaw movement. They are commonly accompanied by jaw pain, clicking, popping, morning jaw stiffness, teeth grinding, or ear discomfort.
What role does the trigeminal nerve play in migraine and TMJ pain?
The trigeminal nerve carries pain signals from the face, jaw, and head to the brain. In migraine, it becomes neurologically activated, while in TMJ disorder, it may be mechanically irritated. This shared involvement explains why the two conditions frequently overlap.
Should I see a neurologist if I have both migraine and jaw pain?
Yes, If headaches are frequent, severe, or accompanied by symptoms such as nausea, light sensitivity, or visual disturbances, a neurologist can evaluate whether migraine, TMJ disorder, or both are contributing to your symptoms and recommend appropriate treatment.
Recent Posts