
Why Do Migraines Make You Nauseous? The Brain-Gut Connection Explained
Why Do Migraines Make You Nauseous? The Brain-Gut Connection Explained Usually severe migraine nausea and vomiting disrupts daily routines and reduces quality of life. Many patients complain that stomach symptoms feel as intense as head pain. Medical research shows that up to 80% of migraine patients experience nausea, and nearly 50% report vomiting during attacks (American Migraine Foundation). Understanding of the migraine gut brain connection helps patients recognize symptoms early and seek proper care. Migraine Nausea And Vomiting Neurological disorders often affect the digestive system more than the brain. Migraine stands out because it impacts both the nervous system and the digestive tract. Many patients notice nausea before migraine pain even begins. That early warning phase is known as the prodrome stage. Migraine digestive symptoms is classified as part of the broader neurological cascade. through complex pathways the brain communicates with the gut. Stomach get upset, delayed digestion, and vomiting is caused due to disruption in those pathways. Key observations from clinical studies: Around 70–80% of patients report nausea About 30–50% experience vomiting Gastrointestinal symptoms often predict migraine severity The Migraine Gut Brain Connection And Its Role In Symptoms The migraine gut brain connection explains the reason why head pain links closely with stomach distress. The brain and gut communicate through the vagus nerve. This acts as a major signaling pathway.Serotonin plays a major role in this process. Nearly 90% of serotonin exists in the gut, not the brain. Changes in serotonin levels affect both mood and digestion. Migraine episodes disrupt serotonin balance, which triggers nausea and slows stomach emptying. Delayed gastric emptying, also called gastroparesis, appears in many migraine patients. Food remains in the stomach longer than normal. That delay leads to bloating, discomfort, and vomiting. Why Migraines Cause Nausea And Vomiting During Attacks Doctors explain why migraines cause nausea through neurological signaling changes. The brainstem becomes highly active during a migraine attack. That area controls vomiting reflexes. Pain signals stimulate regions such as: The hypothalamus The brainstem vomiting center The trigeminal nerve system Activation of those areas leads to migraine nausea and vomiting. Stronger migraines often cause more severe gastrointestinal symptoms. Research from the National Institutes of Health shows that brainstem activation correlates directly with nausea severity in migraine patients. Migraine Nausea Prodrome Symptoms And Early Warning Signs Early detection improves symptom control. Many patients experience migraine nausea prodrome symptoms hours before headache onset. Common early signs include: Mild nausea or queasiness Loss of appetite Fatigue or low energy Sensitivity to smell Recognition of those symptoms allows faster treatment. Early medication use often reduces severity. Migraine Stomach Problems Across Different Phases Migraine affects the digestive system in stages. Each phase presents different symptoms. Prodrome Phase In prodrome phase, Mild nausea before migraine begins. Changes in appetite often occur. Attack Phase In the attack phase severe migraine nausea and vomiting dominate. Patients may struggle to keep food or medication down. Postdrome Phase After headache relief lingering stomach discomfort and fatigue continue. Studies suggest that over 60% of patients report digestive symptoms across multiple phases, not just during peak pain. Migraine Vomiting Relief And Treatment Options Effective migraine vomiting relief requires a combination of medical and lifestyle strategies. Treatment depends on symptom severity and frequency. Medical Treatments Doctors often recommend: Antiemetic medications (ondansetron, metoclopramide) Triptans for migraine control Preventive therapies for chronic cases Lifestyle Strategies Small changes in life of patients may benefit him: Small, frequent meals Hydration with electrolyte fluids Avoidance of trigger foods Telehealth Advantage My Consultant Corner offers fast access to neurologists through virtual visits. Early consultation improves symptom control and reduces emergency visits. [Add Internal Link Here – Tele-neurology Consultation Page] When Medical Attention Becomes Necessary Certain symptoms require immediate medical evaluation. Delayed care can increase complications. Seek medical help if: Severe vomiting leads to dehydration Migraine pattern changes suddenly Confusion or weakness appears Vision loss or speech difficulty occurs Symptoms persist beyond 72 hours Early diagnosis improves long-term outcomes. Telehealth services allow quick access without travel delays. Practical Tips For Managing Migraine Digestive Symptoms Patients can reduce migraine digestive symptoms with consistent habits. Helpful approaches: Maintain regular meal schedules Track triggers in a symptom journal Limit caffeine and alcohol intake Use prescribed medications early Clinical data shows that trigger management reduces migraine frequency by up to 30% in many patients. How My Consultant Corner Supports Migraine Patients Specialized care improves results. My Consultant Corner provides personalized treatment plans tailored to each patient. Services include: Expert neurological evaluation Customized migraine treatment plans Convenient telehealth visits Fast appointment availability Patients gain access to accurate diagnosis and ongoing support. Frequently Asked Questions About Migraine Nausea And Vomiting What causes nausea during a migraine? Brainstem activation and serotonin imbalance trigger stomach symptoms. Can nausea start before head pain? Yes. Many patients report nausea before migraine during the prodrome phase. Why do migraines make you throw up? Strong neurological signals activate the vomiting center in the brain. How long does migraine nausea last? Symptoms may last several hours or continue through all migraine phases. What helps migraine vomiting relief quickly? Antiemetic medications and early migraine treatment provide the fastest relief. Are migraine stomach problems common? Yes. Studies show that most migraine patients experience digestive symptoms. Can telehealth help manage migraines? Yes. Virtual consultations provide fast diagnosis and treatment adjustments. When should medical care be considered? Medical attention is necessary for severe symptoms, dehydration, or neurological changes. Taking Control Of Migraine Nausea And Vomiting Clear understanding of migraine nausea and vomiting helps patients take proactive steps. The migraine gut brain connection explains why symptoms extend beyond head pain. Early recognition, proper treatment, and expert care make a significant difference. My Consultant Corner provides accessible, patient-centered neurological care through telehealth. Quick consultation can reduce symptoms and improve daily life. Ready to take control of migraine symptoms? Schedule a consultation with My Consultant Corner today and receive expert guidance tailored to individual needs.
Post-Stroke Recovery & Rehabilitation

How the Brain Heals and What Truly Drives Recovery A Neurologist-Guided, Patient-Centered Roadmap Stroke Recovery Is a Neurological Process — Not a Waiting Period A stroke is not simply a sudden medical event; it is a neurological injury that disrupts the brain’s ability to control movement, speech, cognition, behavior, and vital bodily functions. Whether caused by an ischemic blockage or an intracerebral hemorrhage, stroke results in acute damage to brain tissue followed by a complex and evolving recovery process. In the United States, nearly 800,000 people experience a stroke each year, making it one of the leading causes of long-term neurological disability. Advances in acute stroke treatment have significantly improved survival. However, survival is only the beginning. What follows is a prolonged and highly individualized process of neurological recovery. For patients and families, this phase is often filled with uncertainty:Will strength return? Will speech improve? How long does recovery take? Is rehabilitation truly effective? From a neurological standpoint, recovery is best understood through two core principles: Stroke recovery is driven by brain plasticity, not time alone Rehabilitation is an active neurological treatment, not supportive care Understanding these principles helps patients and caregivers move forward with clarity, realistic expectations, and hope. How the Brain Heals After Stroke: Understanding Neuroplasticity When a stroke occurs, part of the brain is injured or deprived of blood flow, leading to loss of neurons and disruption of neural networks. Importantly, this injury does not mean the brain is incapable of recovery. Instead, recovery depends on how surviving brain regions adapt over time — a process known as neuroplasticity. What Is Neuroplasticity? Neuroplasticity refers to the brain’s ability to reorganize, strengthen existing connections, and form new neural pathways in response to injury and experience. After a stroke, unaffected areas of the brain can partially assume functions previously handled by damaged regions. This biological adaptability is the foundation of rehabilitation. Crucially, neuroplasticity is activity-dependent. The brain does not reorganize simply with rest or time. Recovery is driven by repetitive, meaningful, task-specific practice, which is why structured rehabilitation is so effective. Early and Late Brain Recovery In the first days to weeks after a stroke, the brain enters a period of heightened plasticity. Swelling subsides, inflammation decreases, and neural signaling stabilizes. During this phase, early improvements may reflect recovery of stunned but viable tissue. While the most rapid gains often occur within the first 3–6 months, recovery does not stop there. Research shows that meaningful improvement can continue for 6–12 months and beyond, particularly when rehabilitation remains progressive and goal-directed. Later recovery often involves: Refinement of motor control rather than large strength gains Improved balance, coordination, and endurance Gradual improvements in language and cognition Development of compensatory strategies that enhance independence The idea that recovery “plateaus” early is often a reflection of reduced therapy intensity or lack of reassessment — not a true limit of neurological potential. Rehabilitation Therapies That Drive Recovery Stroke rehabilitation is not a single therapy or a one-size-fits-all program. It is a multidisciplinary neurological intervention designed to retrain the brain by engaging impaired neural networks repeatedly and purposefully. Physical Therapy: Restoring Mobility and Balance Physical therapy focuses on improving strength, coordination, balance, and gait. Weakness, spasticity, and impaired balance are common after a stroke and significantly affect independence. Through task-oriented and repetitive movement training, physical therapy helps the brain re-map motor pathways, reduce fall risk, and improve functional mobility. Therapy evolves — from basic transfers to higher-level balance, endurance, and community mobility. Occupational Therapy: Regaining Independence in Daily Life Occupational therapy helps patients regain the ability to perform activities of daily living, such as dressing, bathing, eating, writing, and managing household tasks. Stroke often affects fine motor control, visual-spatial processing, and executive function — all critical for daily independence. OT integrates motor, sensory, and cognitive systems, reinforcing purposeful use of affected limbs and promoting functional recovery rather than learned non-use. Speech and Language Therapy: Communication and Swallowing Stroke can affect language (aphasia), speech clarity (dysarthria), cognition, and swallowing (dysphagia). Speech-language therapy addresses: Language comprehension and expression Speech articulation and voice control Cognitive-communication skills Swallowing safety and nutrition Recovery in this domain may be gradual, but meaningful gains can continue long after motor recovery stabilizes. Early swallowing evaluation is essential to reduce aspiration risk and medical complications. Cognitive Rehabilitation: Attention, Memory, and Executive Function Cognitive changes after stroke are common and frequently underrecognized. Patients may struggle with attention, memory, processing speed, or executive skills — even when physical recovery appears strong. Cognitive rehabilitation helps patients develop new strategies to strengthen preserved neural pathways and compensate for deficits. Recovery in this domain often continues later into the recovery process, reinforcing the importance of ongoing reassessment. Early Recovery: The First Weeks Matter — But Don’t Define Everything The first days to weeks after a stroke represent a critical window of opportunity. During this phase, early mobilization and rehabilitation — when medically appropriate — improve functional outcomes and reduce complications. That said, early appearance does not define long-term outcome. Neurologists caution against premature prognostication. Patients may appear severely impaired early on yet make meaningful gains over time, while others with milder strokes may struggle due to secondary complications. Common early challenges include: Fatigue Fluctuating weakness or tone Speech or swallowing difficulty Cognitive slowing or confusion Emotional distress These challenges are common and treatable. Addressing them early improves participation in rehabilitation and long-term outcomes. What Really Predicts Stroke Recovery Recovery is shaped by multiple interacting factors — not a single variable. What Matters Most: Quality, timing, and intensity of rehabilitation Patient engagement and education Ongoing neurological oversight Social and caregiver support Management of medical and neurological complications What Matters Less Than Commonly Believed: Age alone (older adults retain neuroplastic capacity) Early severity as a fixed predictor Arbitrary recovery timelines From a neurologist’s perspective, trajectory over time is far more meaningful than a single snapshot. Cognitive, Emotional, and Behavioral Recovery Physical recovery is often the most visible aspect of stroke rehabilitation, but cognitive and emotional changes can be equally impactful. Cognitive Changes Difficulties with attention, memory, executive function, or visual-spatial processing may affect independence, work, and social engagement. These deficits may emerge
7 Subtle Stroke Signs in Women You Might Be Missing
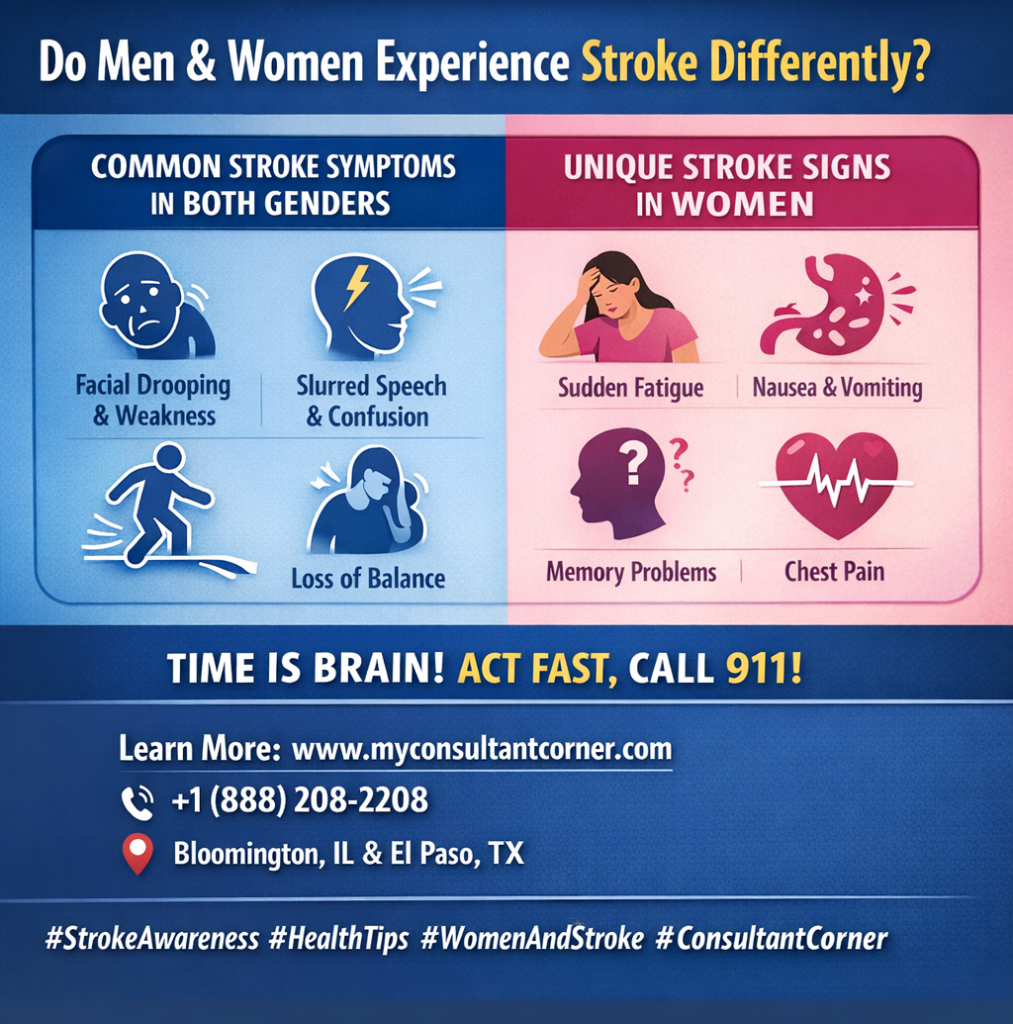
Do Men and Women Experience Stroke Differently? While the core mechanics of a stroke remain the same, clinical data show significant differences in how symptoms manifest based on gender. According to the World Stroke Organization (WSO), women are not only more likely to experience a stroke in their lifetime. Still, they are also 11% more likely to report non-traditional symptoms that lead to delayed diagnosis. Understanding these nuances is vital because every 60 seconds of delayed treatment results in the death of nearly 2 million brain cells. What Common Symptoms Are Shared by Both Genders? In the majority of cases, both men and women will display the “classic” neurological deficits associated with brain cell death. These symptoms are primarily focused on motor skills and sensory processing: Sudden Asymmetry: Drooping of the face, or paralysis of the arm or leg—typically isolated to one side of the body. Cognitive & Sensory Disruptions: Slurred speech, sudden confusion, vision loss, or a severe headache with no identifiable cause. Mobility Issues: Difficulty walking or a sudden loss of balance (the “B” in the BE FAST protocol). Why Are Stroke Signs Frequently Missed in Women? Women are more likely to present with “subtle” or nonspecific symptoms, which are often mistakenly attributed to stress, exhaustion, or other minor ailments. This diagnostic gap is a leading cause of poorer outcomes for female patients. Common “Non-Traditional” Symptoms in Women: Systemic Weakness: A feeling of generalized exhaustion or extreme fatigue that comes on suddenly. Gastrointestinal & Respiratory Signs: Nausea, vomiting, hiccups, or shortness of breath. Altered Mental Status: Disorientation, sudden memory problems, or acting “out of character”. Cardiac Mimics: Chest pain, palpitations, or a racing heartbeat that can sometimes be confused with a heart attack. Which Symptoms Are Relatively More Common in Men? Research suggests men are more likely to exhibit specific coordination and sensory issues. While these are still “classic” signs, they appear with higher frequency in male patients: Ataxia: A sudden, noticeable loss of coordination in the limbs or an unsteady gait. Paresthesia: Distinct sensations of numbness, tingling, or “pins and needles”. Visual Disturbances: Higher reported rates of double vision or sudden dimming of sight in one eye. How Does Gender Affect Treatment Timing and Survival? Feature Statistical Impact on Women Impact on Recovery Recognition Nonspecific signs (nausea, fatigue) lead to frequent misdiagnosis. Delayed treatment. Response Time Women wait an average of 30 to 60 minutes longer to call 911. Increased brain damage. Age of Onset Women typically have strokes at an older age than men. Higher risk of mortality. Disability Risk Women face a higher rate of long-term nursing home placement post-stroke. Reduced independence. When Should You Seek Emergency Help? Regardless of sex, any sudden combination of these symptoms—even if they seem mild or resolve after a few minutes—must be treated as a medical emergency. Call Emergency Services (911): Do not wait for a clinic appointment or try to “sleep it off”. Trust Your Instincts: If a woman reports feeling “not right” combined with sudden fatigue or confusion, seek help immediately. Time is Brain: Accessing clot-busting therapies within the first 3–4.5 hours is the most effective way to prevent permanent disability. Your Recovery Doesn’t End at the Hospital Doors At Consultant Corner, we believe that surviving a stroke is only the beginning. We treat stroke recovery as a continuous journey, not a one-time medical event. Our specialized neurology team offers personalized, data-driven post-stroke care through both convenient virtual consultations and in-person clinic visits. We focus on neuroplasticity, secondary prevention, and restoring your independence. Take the Next Step Toward Healing If you or a loved one needs expert guidance on the path to recovery, our team is ready to support you. Visit: www.myconsultantcorner.com Call: +1 (888) 208-2208 Email: info@myconsultantcorner.com Address: 1404 Eastland Dr, Bloomington, IL 61701, United States Address: 5140 Montana Ave, El Paso, TX 79903, United States
5 Early Stroke Symptoms You Can’t Ignore (2026 Update)
What Are the Main Warning Signs of a Stroke? A stroke happens when blood flow to a part of the brain is interrupted, leading to brain cell damage within minutes. Recognizing the early warning signs can save your life or someone else’s. According to the World Health Organization (WHO), stroke is the second leading cause of death globally, responsible for over 12 million cases every year. Time is critical—knowing the signs and acting fast can reduce the risk of long-term disability and improve recovery outcomes. How Can You Identify Stroke Symptoms Quickly? (Remember: BE FAST) Medical experts use the BE FAST acronym to help people quickly recognize stroke symptoms. Each letter stands for a potential warning sign: B – Balance: Is There Sudden Dizziness or Loss of Coordination? If someone suddenly can’t walk straight, feels dizzy, or loses coordination, it could be an early stroke sign. Research from the American Stroke Association (ASA) suggests that around 40% of stroke patients experience balance problems or sudden dizziness. E – Eyes: Is There Trouble Seeing Clearly? Watch for blurred vision, double vision, or complete vision loss in one or both eyes. About 20% of stroke victims report sudden vision changes, which may appear alongside light sensitivity or visual field loss. F – Face: Is One Side Drooping? Ask the person to smile. If one side droops or feels numb, it’s a red flag. Facial asymmetry is one of the most common early signs of stroke and appears in over 60% of cases according to clinical data. A – Arm: Do the Arms Feel Weak or Numb? Have them raise both arms. If one arm drifts downward or can’t be lifted, that’s a strong indicator of a stroke. This weakness may also affect one leg, typically on the same side. S – Speech: Is the Speech Slurred or Confusing? Speech problems—like slurred words, difficulty understanding, or trouble finding the right words—often signal a stroke. Studies find that nearly 70% of stroke patients present some form of speech impairment at onset. T – Time: Why Is Every Minute Critical? If any of these signs appear, call emergency services immediately. Never wait for the symptoms to improve on their own. Each passing minute can cause an estimated 1.9 million brain cells to die, increasing the risk of permanent brain injury. What Are Other Sudden Symptoms Not to Ignore? Not every stroke follows the same pattern. Some people experience less common, but equally serious symptoms such as: Sudden, severe headache without a known cause—especially if it comes out of nowhere. Loss of consciousness, fainting, or seizure. Nausea, vomiting, or vertigo (a spinning sensation). Sudden confusion or trouble understanding speech. Always treat these as potential emergencies—even if symptoms fade after a few minutes. Why Is Early Recognition of Stroke So Important? When it comes to stroke, every minute truly counts. Each second of delay means more brain cells are lost, and long-term complications become more likely. The World Health Organization (WHO) reports that strokes cause over 6.5 million deaths globally each year, and the risk of severe disability rises sharply with every lost minute of treatment time. In short, the faster a stroke is recognized and treated, the better the outcome. Why Does Fast Action Improve Access to Treatments? Stroke treatments are highly time-sensitive. Clot-busting drugs (known as thrombolytics, such as tPA) and mechanical clot removal procedures must be given within 3 to 6 hours from symptom onset to be most effective. When strokes are recognized quickly: Patients reach CT scans faster, helping doctors confirm the stroke type (ischemic or hemorrhagic). Life-saving therapies can be started sooner, limiting brain damage. Supportive care (like managing blood pressure, oxygen, and glucose) can prevent secondary complications such as brain swelling or infection. In contrast, delayed recognition may mean missing the treatment window entirely, reducing the chance of recovery. How Does Early Recognition Improve Survival and Recovery? Evidence is clear: faster diagnosis leads to better survival and long-term independence. A large-scale study in The Lancet Neurology found that patients treated within the first 90 minutes of a stroke were three times more likely to recover without major disability. Prompt recognition and treatment also mean: Lower mortality rates. Fewer hospital complications, such as blood clots and pneumonia. Greater chances of walking and speaking normally after recovery. Essentially, time to treatment predicts quality of life after stroke. When Should You Go to the ER for a Stroke? If you suspect a stroke—even slightly—call emergency services immediately. Don’t wait to see if symptoms improve, and don’t try to drive yourself. Stroke is a time‑critical medical emergency, and fast action can mean the difference between full recovery and permanent disability. According to the American Heart Association, early treatment within the first few hours can reduce disability by up to 30% and significantly improve survival. The Consultant Corner Approach to Ischemic Stroke At Consultant Corner, we view ischemic stroke as an ongoing recovery process, not a single event. Our neurology team provides personalized post-stroke care through both in-clinic and virtual visits, focusing on recovery, prevention, and long-term brain health. Take the Next Step If you or a loved one is recovering from an ischemic stroke, we’re here to help.Visit www.myconsultantcorner.com, call: +1 (888) 208-2208, or Email: info@myconsultantcorner.com to get started. Address: 1404 Eastland Dr, Bloomington, IL 61701, United States Address: 5140 Montana Ave, El Paso, TX 79903, United States
Syncope & Fainting Spells: Neurological vs Non-Neurological Causes and Expert Care
Syncope & Fainting Spells Neurological vs Non-Neurological Causes, Diagnostic Evaluation, and Expert Care A Comprehensive, Patient-Centered Guide from Consultant Corner Passing out—even briefly—is one of the most unsettling experiences a person can have. Patients often describe fainting spells as sudden, unpredictable, and frightening, while families immediately worry about what it might mean: Was it a seizure? A heart rhythm problem? A stroke? That uncertainty is understandable, because “passing out” can represent everything from a benign reflex episode to a potentially life-threatening cardiac condition—or a neurological event that was mistaken for fainting. Clinically, syncope is common and frequently prompts urgent medical evaluation. It accounts for approximately 1–3% of emergency department visits and up to 6% of hospital admissions, highlighting both its prevalence and the challenge of safely identifying high-risk patients. Over a lifetime, at least one-third of individuals will experience syncope, with incidence rising again in older adulthood—precisely the population at greatest risk for injury, medication interactions, autonomic dysfunction, and cardiac disease. In many cases, patients are reassured quickly and discharged without a clear explanation. Sometimes that reassurance is appropriate. In other cases, however, premature diagnostic closure can miss a serious underlying condition or delay appropriate follow-up. The central challenge is that syncope is not a diagnosis—it is a symptom. It reflects a brief, reversible reduction in blood flow to the brain, and the clinician’s task is to determine why that reduction occurred and whether the patient is at risk of recurrence, injury, or sudden deterioration. From a neurologist’s perspective, fainting spells sit at the crossroads of neurology, cardiology, and autonomic physiology. Many events described as “fainting” are not true syncope at all, but rather neurological mimics such as seizures or transient alterations in awareness. At the same time, some of the most dangerous causes are cardiac and may present with little or no warning. The goal of evaluation is to separate neurological from non-neurological causes, identify red flags early, and pursue targeted—not excessive—testing. At Consultant Corner, we approach syncope as a diagnostic problem that deserves clarity, evidence-based reasoning, and individualized care. Whether an episode represents vasovagal syncope, orthostatic hypotension, arrhythmia, seizure, or autonomic dysfunction, our focus is on helping patients understand what happened, what risks matter, and how to move forward safely. What Is Syncope — and Why the Brain Is Central Syncope is defined as a transient loss of consciousness due to temporary, global cerebral hypoperfusion, followed by rapid and complete recovery. In practical terms, fainting occurs when the brain is briefly deprived of sufficient oxygen and glucose to maintain consciousness. Unlike coma or traumatic brain injury, syncope does not involve permanent brain damage; however, it signals a failure in the systems that normally sustain cerebral perfusion. The brain is uniquely sensitive to even small changes in blood pressure and cardiac output. Consciousness depends on tightly regulated interactions between the heart, blood vessels, and autonomic nervous system. When these systems fail—due to sudden hypotension, abnormal heart rhythm, impaired autonomic reflexes, or volume depletion—cerebral perfusion can fall below a critical threshold within seconds, resulting in collapse. What makes syncope challenging is that it represents a final common pathway rather than a single disease. Unlike seizures or strokes, syncope does not originate from intrinsic electrical or structural brain pathology. Instead, it reflects failure of the physiological support systems that maintain brain function. In clinical practice, however, this distinction is often blurred, as neurological disorders may mimic syncope, trigger syncope, or coexist with non-neurological causes. Neurological vs Non-Neurological Causes: Why the Distinction Matters One of the most important steps in evaluating fainting spells is determining whether the underlying cause is neurological or non-neurological. This distinction directly shapes diagnostic testing, treatment decisions, long-term risk assessment, and patient counseling. From a neurologist’s standpoint, the priority is not merely confirming that syncope occurred, but ensuring that neurological conditions are not overlooked, particularly those that masquerade as syncope or present with transient loss of consciousness as a secondary manifestation. At the same time, it is equally important to recognize when fainting is driven by cardiac or systemic disease that carries its own risks. Because symptoms often overlap and witness descriptions are frequently incomplete, fainting spells require a structured, neurologist-led approach that integrates neurological, cardiovascular, and autonomic factors rather than evaluating them in isolation. Neurological Causes and Neurologic Mimics of Syncope Seizures: The Most Clinically Significant Mimic Distinguishing syncope from epileptic seizures is one of the most consequential challenges in evaluation. Both can present with sudden collapse and loss of consciousness, but the safety implications, driving restrictions, employment, and long-term management differ substantially. Seizures arise from abnormal, hypersynchronous electrical activity in the brain and are typically followed by a post-ictal period characterized by confusion, fatigue, headache, or focal neurological deficits. Syncope, in contrast, results from transient cerebral hypoperfusion and is usually followed by rapid recovery once blood flow is restored. In practice, overlap is common. Syncope may be accompanied by brief involuntary movements due to brainstem hypoxia (convulsive syncope), while some seizures may be brief or subtle and lack dramatic convulsions. Because missing a seizure diagnosis carries serious consequences, careful neurological assessment is essential, and EEG or prolonged monitoring may be required when history alone is insufficient. Autonomic Nervous System Disorders and Neurogenic Syncope The autonomic nervous system continuously regulates blood pressure, heart rate, and vascular tone in response to posture, stress, and exertion. Disorders affecting this system can impair the body’s ability to maintain cerebral perfusion, leading to recurrent or unexplained syncope. Neurological conditions associated with autonomic failure include Parkinson’s disease and related neurodegenerative disorders, multiple system atrophy, diabetic autonomic neuropathy, small fiber neuropathies, and other disorders involving peripheral or central autonomic pathways. In recent years, post-viral and post-COVID dysautonomia have emerged as increasingly recognized causes of syncope and orthostatic intolerance, particularly in younger patients without structural heart disease. Neurogenic syncope is often posture-dependent, recurrent, and accompanied by other autonomic symptoms such as heat intolerance, gastrointestinal dysmotility, urinary dysfunction, or abnormal sweating. Diagnosis frequently requires specialized autonomic testing and longitudinal neurological care, rather than episodic reassurance. Structural and Cerebrovascular Neurological Considerations Although uncommon, certain structural or vascular neurological conditions can present with transient loss of consciousness.
Hand Numbness & Carpal Tunnel Syndrome | When to See a Neurologist

Carpal Tunnel Syndrome & Nerve Entrapment Disorders Understanding Symptoms, Diagnosis, and When Neurological Evaluation Matters A Patient-Centered, Evidence-Based Guide from Consultant Corner Numbness, tingling, pain, or weakness in the hands and arms are among the most common neurological complaints encountered in outpatient practice. Patients often describe their hands “falling asleep,” waking at night with burning or pins-and-needles sensations, dropping objects unexpectedly, or struggling with fine motor tasks such as typing, writing, or buttoning clothes. These symptoms can be disruptive, frightening, and persistent — and they often raise an important question: Is this something serious? Carpal tunnel syndrome is frequently the first diagnosis patients encounter when they search for answers online. It is indeed common, affecting an estimated 3–6% of adults, and it represents the most frequent peripheral nerve entrapment disorder. However, not all hand numbness is carpal tunnel syndrome, and not all nerve symptoms originate at the wrist. From a neurologist’s perspective, symptoms involving the hands and arms sit at the intersection of peripheral nerve anatomy, spinal health, systemic disease, occupational factors, and individual anatomy. This complexity explains why nerve entrapment disorders are sometimes dismissed too quickly — or, conversely, overdiagnosed and overtreated. Accurate diagnosis requires careful localization, clinical reasoning, and, in many cases, objective testing. At Consultant Corner, we approach carpal tunnel syndrome and related nerve entrapment disorders with a structured, evidence-based neurological framework designed to provide clarity, reassurance, and appropriate care. Understanding Nerve Entrapment: A Neurological Perspective Peripheral nerves travel long distances from the spinal cord to the muscles and skin, passing through narrow anatomical corridors formed by bones, ligaments, and soft tissue. At certain predictable locations, these nerves are vulnerable to compression. Even modest increases in pressure — due to inflammation, fluid retention, repetitive motion, or structural crowding — can disrupt nerve blood flow and electrical signaling. This process, known as nerve entrapment, typically develops gradually. Early symptoms are often sensory, such as intermittent tingling or numbness. If compression persists, symptoms may become constant and progress to weakness, coordination difficulty, or muscle atrophy. Importantly, symptoms are not always felt at the site of compression, which is why localization based on anatomy — rather than symptom location alone — is central to diagnosis. Carpal Tunnel Syndrome: Common, but Often Misunderstood Carpal tunnel syndrome results from compression of the median nerve as it passes through the carpal tunnel at the wrist. This tunnel is a rigid, confined space, and it has very little capacity to accommodate swelling or structural change. As pressure increases, the median nerve becomes vulnerable to dysfunction. Patients with carpal tunnel syndrome typically experience numbness, tingling, or burning sensations in the thumb, index finger, middle finger, and part of the ring finger. Symptoms often worsen at night or during activities involving sustained wrist positioning. Many patients report relief by shaking or repositioning the hand — a classic feature that reflects temporary restoration of nerve blood flow. As compression progresses, patients may develop weakness of thumb movements, difficulty with fine motor tasks, or frequent dropping of objects. These signs suggest more advanced nerve involvement and warrant timely evaluation. A key anatomical clue is that carpal tunnel symptoms usually spare the little finger, which is supplied by a different nerve. Carpal tunnel syndrome may exist on its own, but it can also coexist with cervical spine disease or generalized neuropathy — a phenomenon sometimes referred to as double crush syndrome. In these cases, symptoms may be more severe or less responsive to isolated wrist treatment, reinforcing the importance of a comprehensive neurological assessment. Other Nerve Entrapments That Mimic Carpal Tunnel Syndrome While carpal tunnel syndrome is the most common diagnosis, many patients referred for “carpal tunnel–like” symptoms ultimately have nerve compression at a different site, or at multiple sites. The ulnar nerve, for example, is frequently compressed at the elbow in cubital tunnel syndrome. This condition typically causes numbness in the ring and little fingers, hand weakness, and symptoms worsened by prolonged elbow flexion or pressure. Compression can also occur at the wrist in Guyon’s canal, producing a different but related symptom pattern. The radial nerve may be compressed in the forearm, leading to pain or weakness of wrist and finger extension, often without prominent sensory symptoms. In the lower extremities, compression of the peroneal nerve near the knee can cause foot drop, while tarsal tunnel syndrome involves compression of the posterior tibial nerve at the ankle, producing burning or tingling in the sole of the foot. These conditions illustrate why accurate localization matters. Treatments that help carpal tunnel syndrome may not improve symptoms caused by ulnar or radial nerve compression, and unnecessary procedures can be avoided with careful neurological evaluation. Neurological, Orthopedic, and Systemic Contributors: Why Symptoms Overlap Hand and limb symptoms do not always arise from focal nerve entrapment. Orthopedic conditions such as arthritis or tendon disease may cause pain and stiffness that limit function but do not follow nerve distributions. Systemic conditions — including diabetes, thyroid disease, vitamin deficiencies, autoimmune disorders, and medication effects — can produce diffuse nerve dysfunction that mimics entrapment. Neurologists differentiate these possibilities by focusing on pattern recognition: nerve-specific sensory changes, reflex alterations, weakness patterns, and progression over time. This distinction is critical because treating a single compression site will not resolve symptoms driven by a systemic process. When Symptoms Should — and Should Not — Raise Concern Many nerve entrapment symptoms are intermittent and reversible, especially early in their course. Tingling that occurs primarily at night, symptoms triggered by certain positions, or discomfort relieved by rest or splinting are often signs of functional nerve compression rather than permanent damage. However, persistent numbness, progressive weakness, visible muscle thinning, or loss of fine motor control warrant earlier neurological evaluation. Rapid progression, involvement of multiple limbs, or symptoms extending beyond a single nerve distribution raise concern for more proximal or systemic conditions. From a neurological standpoint, duration and progression matter more than intensity alone. Early evaluation allows for intervention before nerve injury becomes irreversible. How Nerve Entrapment Is Diagnosed A careful neurological examination remains the cornerstone of diagnosis. By assessing sensation, strength, reflexes, coordination, and muscle bulk, neurologists can often localize nerve
Epilepsy and Seizures: Diagnosis, Treatment, and Quality of Life

What Is Epilepsy and How Can It Change Your Life? Hey there, if you’ve ever wondered about epilepsy, you’re not alone. It’s one of the most common neurological conditions out there, affecting around 50 million people worldwide according to the World Health Organization. In the US alone, about 2.9 million adults live with active epilepsy—that’s roughly 1% of the adult population, per CDC data from 2021-2022. And get this: 1 in 26 people will develop epilepsy at some point in their life. But epilepsy isn’t just about dramatic seizures; it’s a complex brain disorder that touches everything from your daily routine to your long-term health. Let’s break it down in a way that’s easy to follow, like we’re chatting over coffee. Understanding Seizures vs. Epilepsy: What’s the Real Difference? First things first—seizures and epilepsy aren’t the same thing, and mixing them up can lead to confusion. A seizure is like a sudden electrical storm in your brain, often triggered by things like infections, injuries, or even alcohol withdrawal. But epilepsy? That’s when you have an ongoing tendency for unprovoked seizures. Research shows the annual incidence of epilepsy is about 61-68 cases per 100,000 people globally, based on meta-analyses from studies like those in the Neurology journal. If you’ve had just one seizure, it doesn’t automatically mean epilepsy. In fact, rushing to that label could mean unnecessary meds and stress. On the other hand, delaying a diagnosis may leave you vulnerable to additional risks. Think about it: accurate diagnosis helps predict recurrence—studies indicate that after a first unprovoked seizure, the risk of another can be as high as 40-50% without treatment. Why Is Epilepsy Considered a Brain Network Disorder? Epilepsy isn’t about one rogue neuron; it’s a whole network gone haywire. Your brain’s excitability increases, leading to those abnormal syncs. Causes vary—structural issues like strokes or tumors, genetic factors, inflammation, or even unknowns. Data from the Global Burden of Disease Study 2021 estimates 51.7 million people globally deal with this, with a prevalence of around 658 per 100,000. This network view explains why epilepsy looks different for everyone. Some have focal seizures starting in one brain area, while others are more widespread. Personalized care is key because, as research highlights, treating it like a one-size-fits-all just doesn’t cut it. How Do Epilepsy Seizures Really Show Up in Everyday Life? Forget the movie stereotypes—epilepsy seizures aren’t always full-body convulsions. Many are subtle: a brief stare, lip smacking, or that weird déjà vu feeling. Absence seizures in kids might just look like daydreaming, lasting seconds. These can mimic other issues like anxiety or migraines, leading to misdiagnosis. Witness accounts and your own story often tell more than tests. And stats back this: epilepsy affects all ages, but in older adults, new seizures often signal strokes or medication interactions. Early recognition matters because uncontrolled seizures disrupt work, school, and safety. Diagnosing Epilepsy: How Do We Get It Right Over Time? Diagnosing epilepsy is more art than science sometimes—it’s clinical, backed by tools like EEGs and MRIs. A normal EEG doesn’t rule it out, though; up to 50% of people with epilepsy have normal readings between seizures. Genetic tests or video monitoring help in tough cases. The process evolves with follow-ups. Longitudinal studies show that precise diagnosis boosts outcomes, reducing unnecessary treatments and improving life quality. Treating Epilepsy: Why Medication Adherence Is Your Best Friend For most with epilepsy, meds are the go-to. About 70% of people can achieve seizure freedom with proper treatment, per WHO findings. We pick based on your seizure type, age, and lifestyle—considering side effects and even pregnancy plans. But adherence? That’s huge. Missing doses causes breakthrough seizures, a top reason for ER visits. Research from longitudinal cohorts shows 50.5% get seizure-free on the first med, but consistency keeps it that way. Let’s talk openly about side effects; adjusting thoughtfully prevents bigger issues. How Do Anti-Seizure Meds Work in Managing Epilepsy? These meds tweak brain excitability—some block sodium channels to calm firing, others boost calming signals like GABA. Newer ones target multiple paths, expanding options for better control with fewer side effects. Data from 30-year studies: After the first med, about half achieve freedom; second tries bump it up. But lapses drop blood levels, spiking risks. Addressing adherence early avoids labeling as “drug-resistant” prematurely. What Happens with Drug-Resistant Epilepsy and Next Steps? If two meds fail—defining drug-resistant epilepsy, affecting 25-30% per NINDS—don’t just swap endlessly. That’s when specialized centers shine. Early referral cuts side effects and boosts chances. Studies show continued med tweaks alone rarely lead to freedom; advanced options do better. Advanced Epilepsy Treatments: From VNS to Surgery For tough epilepsy cases, tech steps in. Vagus nerve stimulation (VNS) cuts seizures by 50%+ over time, improving mood too. Responsive neurostimulation (RNS) or deep brain stimulation (DBS) disrupts bad activity on demand. Surgery? For focal epilepsy, it offers 70-75% seizure freedom rates, per Yale Medicine research, higher than laser ablation’s 60%. Advances in imaging make it safer, expanding who qualifies. Living with Epilepsy: Boosting Cognition, Safety, and Quality of Life Epilepsy hits more than seizures—it affects your mind, mood, and daily vibe. Quality of life (QoL) scores for people with epilepsy average around 55-60 out of 100, lower than norms, per studies like those in BMJ Open. Factors? Frequent seizures, med side effects, and comorbidities like depression (40% more likely in new diagnoses, AES research). Anxiety, fatigue, and sleep issues are common. Driving bans or job worries add stress, but planning helps. Proactive check-ins maintain independence—data shows better QoL with controlled seizures. Epilepsy Across Your Lifespan: Tailored Care for Every Stage Epilepsy shifts with age. Kids face school hurdles; adults, work and health links; seniors, higher risks from strokes. Age-standardized data from the Lancet show varying burdens, so reassess regularly for safety. Future Advances in Epilepsy Care: What’s on the Horizon? Epilepsy care is booming—high-res imaging, genetics, AI for EEGs, wearables for detection. Research from UCB and others targets refractory cases, aiming for precision. Stats: 75% now control seizures with
How to Achieve the Best Night’s Sleep: Science-Backed Tips That Work

How Can You Achieve the Best Night’s Sleep Possible? Hey there, if you’re tossing and turning at night or waking up feeling like you barely rested, you’re not alone. More than one in three U.S. adults doesn’t get enough sleep, which can lead to serious health issues like increased risk of depression and anxiety. But the good news? With some simple tweaks backed by science, you can unlock the best night’s sleep and wake up energized. Let’s break it down step by step, drawing from research like CDC guidelines and studies from the Sleep Foundation, to make this feel like a chat over coffee rather than a lecture. Why Does a Consistent Schedule Deliver the Best Night’s Sleep? Sticking to the same bedtime and wake-up time every day—even on weekends—is like training your body’s internal clock for peak performance. This aligns with your circadian rhythm, making it easier to drift off and stay asleep. Research from the National Sleep Foundation shows that irregular sleep patterns increase the odds of metabolic syndrome by 23% for every hour of variability in sleep timing. In fact, about 70% of U.S. adults aren’t getting consistent sleep, leading to higher risks of obesity, heart disease, and even poorer mental health. So, pick times that give you 7-9 hours (the sweet spot for most adults, per CDC data), and watch how your energy levels soar. How Can Light Exposure Boost the Best Night’s Sleep? Picture this: starting your day with bright sunlight isn’t just refreshing—it’s a science-backed hack for better rest. Morning light helps strengthen your circadian rhythm, making you feel alert during the day and sleepy at night. Harvard studies emphasize getting natural light early to regulate melatonin, the hormone that signals bedtime. On the other hand, dim the lights in the evening and avoid bright screens, as blue light can reduce melatonin production by up to 50% in some cases. Data shows this simple swap can cut time to fall asleep and increase deep sleep stages. What Makes the Ideal Environment for the Best Night’s Sleep? Your bedroom should feel like a cozy sanctuary, not a cluttered office. Keep it cool—around 60-68°F—as studies from the Sleep Foundation link lower temps to faster sleep onset and fewer wake-ups. Block out light with blackout curtains and noise with earplugs or white noise machines. Research indicates that a quiet, dark space can improve sleep quality by 20-30%, reducing risks like high blood pressure. Don’t forget a supportive mattress and pillows; discomfort is a top culprit for poor rest, affecting up to 25% of adults with chronic sleep issues. How Does a Relaxing Routine Set You Up for the Best Night’s Sleep? Wind down like a pro—think of it as signaling to your brain that it’s time to chill. Spend 30-60 minutes on calm activities like reading or gentle stretching, avoiding thrillers or work emails. A 2013 study found that scents like lavender can calm the nervous system, helping you relax and fall asleep faster. If your mind races, try journaling or deep breathing; techniques like these have been shown to reduce insomnia symptoms by up to 50% in clinical trials. And if you’re still awake after 20 minutes? Get up and do something boring until drowsiness hits—it’s a proven way to avoid associating bed with frustration. Can Exercise Help You Unlock the Best Night’s Sleep? Absolutely—moving your body during the day is a game-changer, but time it right. Regular moderate aerobic exercise, like walking or cycling, is linked to better sleep quality and a 30-50% lower risk of insomnia, according to epidemiologic studies. Aim for activity earlier in the day, as evening workouts can rev you up. Data from chronic exercise research shows it boosts deep sleep stages, improving overall restoration and even mood the next day. What Diet Choices Promote the Best Night’s Sleep? What you eat and drink plays a huge role—skip caffeine after noon, as it can linger and disrupt sleep for hours. Alcohol might knock you out initially, but it fragments rest later, leading to poorer quality, according to Sleep Foundation findings. Opt for light snacks if hungry before bed, avoiding heavy meals that can cause discomfort. Studies show that limiting these can increase sleep efficiency by 10-15%, helping you feel more refreshed. How Do Naps and Screens Impact the Best Night’s Sleep? Short naps (20-30 minutes early in the day) can recharge you without messing up nighttime rest, but long ones? They steal from your sleep drive. As for screens, cut them off an hour before bed—blue light suppresses melatonin, and research ties it to delayed sleep onset in 80% of users. Use night mode or blue-light glasses if you must scroll. Wrapping It Up: Your Path to the Best Night’s Sleep Consistency is your best friend here—start with one or two changes, like a fixed schedule or better light habits, and build from there. If issues persist, chat with a doctor, as conditions like sleep apnea affect millions and can be treated. Prioritizing the best night’s sleep isn’t just nice; it’s essential for health, with data showing it cuts chronic disease risks and boosts mental well-being. Sweet dreams—you’ve got this! When Sleep Problems Persist, Expert Care Matters If you’re experiencing ongoing sleep problems—such as insomnia, excessive daytime fatigue, restless sleep, or suspected sleep disorders—it may be time to seek expert medical guidance. At My Consultant Corner, we provide specialized, patient-centered care led by an experienced Neurologist, focused on identifying the root cause of your sleep concerns and creating an effective, personalized treatment plan. We proudly serve patients in Bloomington, Illinois, and across Texas, offering expert neurological evaluation for sleep disorders in a supportive and professional setting. Don’t let poor sleep affect your health, focus, or quality of life.Take the first step toward better rest and long-term well-being today. 👉 Schedule your consultation with My Consultant Corner now 🌐 Visit: https://myconsultantcorner.com to schedule your sleep‑focused neurology consultation today. 📍 Address: 1404 Eastland Dr, Bloomington, IL 61701, United States 📍 Address:
What Causes Sleep Disorders? 7 Key Reasons (Backed by Science)
What causes sleep disorders? (And what the research really says) If you’ve ever tossed and turned at night, woken up exhausted, or struggled to stay awake during the day, you’re not alone. Around 50–70 million adults in the U.S. have a chronic sleep disorder, and poor sleep costs the economy an estimated $411 billion a year in lost productivity and health issues (CDC, Sleep Foundation). But what’s really behind sleep disorders? It’s rarely just “stress” or “bad habits.” Real causes run deep — from medical conditions and mental health to genes, meds, and even your bedroom setup. Let’s break it down, with real data and practical insights. What medical conditions cause sleep disorders? Many physical health problems directly mess with your ability to sleep well. In fact, studies show that over 80% of people with chronic pain also suffer from insomnia or disrupted sleep (Mayo Clinic, Sleep Medicine Reviews). Chronic pain (arthritis, back pain, fibromyalgia, migraines) makes it hard to fall asleep and stay asleep. Pain signals keep the brain alert, even when the body is tired. Breathing issues like asthma, COPD, allergies, and sinus problems can cause frequent awakenings, especially at night. Heart and lung conditions (heart failure, atrial fibrillation, COPD) are strongly linked to central sleep apnea, where breathing stops and starts during sleep. Neurological disorders such as Parkinson’s, multiple sclerosis, and stroke often disrupt normal sleep patterns and increase the risk of REM sleep behavior disorder. Obesity is a major driver of obstructive sleep apnea. Research shows that people with a BMI over 30 are 5–10 times more likely to develop OSA than those with a healthy weight (American Academy of Sleep Medicine). Diabetes, GERD, and thyroid issues (like hypothyroidism) also contribute to poor sleep quality and nighttime awakenings. Bottom line: If you have a long‑term health condition, it’s worth asking your doctor, “Could this be affecting my sleep?” How mental health affects sleep disorders Mental health is one of the biggest triggers of sleep problems, especially insomnia. Studies show that: 75–90% of people with depression report trouble sleeping. 50–70% of people with anxiety disorders have chronic insomnia. PTSD sufferers are 2–3 times more likely to have nightmares, insomnia, and sleep apnea (Journal of Clinical Sleep Medicine). Common psychological causes include: Stress and anxiety – Work pressure, money worries, relationship issues, or big life changes can keep the mind racing at night. Depression – Often linked to early morning awakenings, trouble falling asleep, and non‑restorative sleep. Trauma and PTSD – Nightmares, night sweats, and hypervigilance make deep, restful sleep nearly impossible. Bipolar disorder and mood disorders – These often come with irregular sleep patterns, like sleeping too much during depressive episodes or too little during manic phases. The cycle is real: poor sleep worsens mental health, and poor mental health worsens sleep. That’s why treating both together (therapy + sleep hygiene) works best. Medications and substances that disrupt sleep Many common drugs and substances interfere with sleep quality, timing, and depth. Research shows that: Up to 30% of chronic insomnia cases are linked to medications or substances (Sleep Medicine Clinics). 20–30% of people with sleep apnea report worsening symptoms after drinking alcohol. Here’s what to watch for: Prescription meds – Some antidepressants, blood pressure drugs, corticosteroids, and ADHD stimulants can cause insomnia or daytime sleepiness. Over‑the‑counter drugs – Cold and allergy medicines, decongestants, and weight‑loss pills often contain stimulants that delay sleep. Caffeine – Even moderate intake (coffee, tea, energy drinks) after 2–3 PM can delay sleep onset by 30–60 minutes and reduce deep sleep. Alcohol – It may help you fall asleep faster, but it fragments sleep, reduces REM sleep, and worsens sleep apnea. Nicotine and recreational drugs – These act as stimulants and can cause frequent awakenings and lighter sleep. Tip: If you’re on any regular meds and having sleep issues, ask your doctor whether they could be contributing. Lifestyle and schedule habits that cause sleep disorders Your daily routine plays a huge role in whether you develop a sleep disorder. Data shows that: Shift workers are 2–3 times more likely to have insomnia or circadian rhythm disorders. People with irregular sleep schedules (bedtime varying by 2+ hours) are 40% more likely to report poor sleep quality (Sleep Health Journal). Key lifestyle causes: Shift work and jet lag – Working nights or rotating shifts throws off your internal body clock, leading to shift work sleep disorder. Inconsistent sleep schedule – Going to bed and waking up at very different times (even on weekends) confuses your circadian rhythm. Poor sleep hygiene – Using phones/tablets in bed, eating heavy meals late, or exercising too close to bedtime can all make it harder to fall and stay asleep. Simple fix: Aim for a consistent bedtime and wake‑up time, even on weekends, and create a relaxing pre‑sleep routine. Environmental and situational factors behind sleep disorders Your bedroom and life events can trigger or worsen sleep problems. Research shows that: Noise, light, and uncomfortable temperatures are among the top reasons people report poor sleep. Acute stress (job loss, moving, divorce, grief) is a common trigger for short‑term insomnia. Common environmental causes: Noise and light – Street noise, snoring partners, or bright screens can prevent deep sleep and cause frequent awakenings. Uncomfortable sleep environment – A bad mattress, wrong pillow, or room that’s too hot or too cold can make it hard to stay asleep. Life stress and trauma – Big life changes, financial stress, or emotional trauma often lead to short‑term insomnia, which can become chronic if not addressed. Quick wins: Keep the bedroom cool, dark, and quiet. Use blackout curtains, earplugs, or a white noise machine if needed. Avoid screens (phones, TV) at least 30–60 minutes before bed. Genetic and biological causes of sleep disorders Some sleep disorders run in families or are tied to brain chemistry. Science shows that: Narcolepsy is strongly linked to a loss of brain cells that produce hypocretin (orexin), and about 10–25% of people with narcolepsy have a family history. Restless legs syndrome (RLS) has a genetic component; if a parent has RLS, the child’s risk is 3–6 times higher. Circadian rhythm disorders (like
How to Wake a Heavy Sleeper (Science-Backed & Easy Tips)
Why Is Waking a Heavy Sleeper So Hard, Honestly? Okay, first things first — it’s not laziness.When someone is a heavy sleeper, their brain is literally offline in the deepest repair mode. During deep sleep (called Stage N3), the brain produces super slow waves. At this point, even loud alarms, shouting, or shaking can feel like background noise to the brain. It’s doing its thing and does not want interruptions. That’s why some people sleep through alarms as if nothing happened. What’s Actually Going On During Deep Sleep? Here’s the behind-the-scenes stuff: Deep sleep makes up about 25% of total sleep The first deep sleep phase lasts 45–90 minutes It mostly happens in the first half of the night During this time: Heartbeat and breathing are at their slowest Muscles are completely relaxed The brain raises its “ignore everything” shield So yeah… waking someone up here is like trying to boot a laptop during a system update. Are Heavy Sleepers Really That Common? Way more than you’d think. Only about 56% of people get the healthy 7–8 hours of sleep.On top of that, sleep disorders affect millions, and the numbers keep rising. Basically, a LOT of people struggle with poor sleep quality — which makes mornings rough, no matter how early the alarm goes off. So if mornings feel like a daily battle, you’re definitely not alone. Why Does Light Work Better Than Sound for Waking Up? Because light speaks the body’s language 🌅 Gradual light exposure tells your brain: “Hey… morning’s coming… time to wake up.” It boosts cortisol naturally (the good, wake-you-up kind), instead of shocking your system. Sunrise alarm clocks or natural sunlight over 15–30 minutes work beautifully — especially if you’re someone who feels dead in the mornings. No jump scare. Just a smooth wake-up. Are Loud Alarms Actually Making Things Worse? Short answer: yes. Studies show that melodic alarms work way better than harsh beeping.People wake up feeling: More alert Less cranky Less foggy Your sleep cycles run in 90–120 minute loops, so if your alarm hits right in deep sleep, you’ll feel awful no matter how loud it is. Timing + gentle sound > aggressive noise. Why Does Getting Out of Bed Help So Much? Movement flips the “wake up” switch fast. Try this: Put your alarm across the room Force yourself to stand up to turn it off Once your body moves: Blood circulation increases Brain alertness rises Sleep fog starts breaking It’s annoying, yes — but effective. Do Vibrating Alarms Actually Work? Surprisingly… yes. Vibration triggers touch receptors, not hearing.That means your brain can’t just ignore it the way it ignores sound. They’re especially good if: You sleep through noise You’re a super deep sleeper Regular alarms do absolutely nothing Think of it as a physical nudge instead of yelling at your ears. Can Temperature or Touch Help Wake Someone Up? Absolutely. Gentle strategies work best: Light pressure on the shoulders or arms Cool air or opening a window Lower room temperature slightly Your body naturally warms up when waking, so temperature contrast helps signal “okay, time to move.” No drama. Just biology doing its job. Do Smells Really Wake People Up? Yes — and it’s kind of cool. The smell system connects directly to the brain’s alert centers.Fresh air, citrus, or minty scents can gently pull someone out of sleep without shocking them. It’s subtle, but when combined with light or movement, it works surprisingly well. Why Do Abrupt Wake-Ups Feel So Terrible? Because your body panics 😬 Sudden alarms can: Spike stress hormones Jolt the heart Leave you groggy for 30–60 minutes That foggy, zombie feeling?That’s sleep inertia, and it’s strongest when you’re dragged out of deep sleep. Which is why smoother wake-ups feel 10x better. So… What’s the Best Way to Wake a Heavy Sleeper? Best-friend advice?Don’t fight the body — work with it. The magic combo: Gradual light Soft or melodic sound Physical movement Cool air or gentle touch Optional scent boost Together, these gently guide the brain out of sleep instead of ripping it awake. When Heavy Sleeping Signals a Sleep Disorder Occasionally sleeping deeply is normal—but consistently struggling to wake up, sleeping through alarms, feeling mentally foggy for hours, or remaining exhausted despite adequate sleep may point to an underlying sleep disorder rather than “just being a heavy sleeper.” Conditions such as insomnia, circadian rhythm disorders, sleep apnea, hypersomnia, and other neurological sleep disturbances can disrupt normal sleep architecture, keeping the brain stuck in deep sleep or preventing restorative rest. Over time, this can affect concentration, mood, work performance, cardiovascular health, and overall quality of life. How MyConsultantCorner Can Help At MyConsultantCorner, we connect patients with experienced neurology specialists who evaluate sleep-related neurological patterns, identify contributing factors, and develop personalized treatment plans—not just quick fixes. Your care may include: A detailed sleep and symptom assessment Review of sleep schedules, fatigue patterns, and morning inertia Evaluation for neurological or circadian rhythm disorders Guidance on evidence-based behavioral and medical treatments Ongoing support through virtual neurology consultations If waking up feels like a daily struggle, or if deep sleep is interfering with your ability to function, early evaluation can make a meaningful difference. Many sleep disorders are highly treatable once properly identified. Take the Next Step Toward Better Sleep You don’t have to accept exhaustion as normal. If heavy sleeping, morning grogginess, or poor sleep quality is affecting your life, professional neurology care can help you regain balance and clarity. Contact MyConsultantCorner today to schedule a sleep-focused neurology consultation and start working toward healthier, more restorative sleep. 🌐 Visit: https://myconsultantcorner.com 📍 Address: 1404 Eastland Dr, Bloomington, IL 61701, United States📞 Call: +1 (888) 208–2208📧 Email: info@myconsultantcorner.com Expert care. Personalized guidance. Better sleep starts here.